
Haemochromatosis revisited
2022-11-29 06:44:46AlineMorganAlvarengaPierreBrissotPauloCalebJuniorLimaSantos
World Journal of Hepatology 2022年11期
Aline Morgan Alvarenga,Pierre Brissot,Paulo Caleb Junior Lima Santos
Abstract
Haemochromatosis is a genetic disease caused by hepcidin deficiency, responsible for an increase in intestinal iron absorption. Haemochromatosis is associated with homozygosity for the HFE p.Cys282Tyr mutation. However, rare cases of haemochromatosis (non-HFE haemochromatosis) can also be caused by path-ogenic variants in other genes (such as HJV, HAMP, TFR2 and SLC40A1). A working group of the International Society for the Study of Iron in Biology and Medicine (BIOIRON Society) has concluded that the classification based in different molecular subtypes is difficult to be adopted in clinical practice and has proposed a new classification approaching clinical questions and molecular complexity. The aim of the present review is to provide an update on classification, pathophysiology and therapeutic recommendations.
Key Words: Haemochromatosis; Iron overload; HFE; Molecular diagnosis; Hepcidin
INTRODUCTION
Haemochromatosis is characterized as systemic iron overload of genetic origin caused by hepcidin deficiency, including decreased production of this hormone or decreased activity of hepcidinferroportin binding[1] (Figure 1). Iron overload leads to damage such as liver cirrhosis, cardiomyopathy, diabetes, arthritis, hypogonadism and skin pigmentation. Therapeutic phlebotomy is effective and safe[2]. Iron chelation, mostly confined to iron overload related to chronic anaemia needing repeated transfusions, is an alternative (or adjuvant) treatment in haemochromatosis, especially when phlebotomies are medically contraindicated[3] or iron overload is so great that iron depletion is urgently needed.
Mostly, the disease is related to homozygosity for the gene HFE p.Cys282Tyr genetic alteration (which is the classical type 1 haemochromatosis). p.Cys282Tyr/p.His63Asp compound heterozygosity has been reported to be linked to haemochromatosis. Rarely, the cases of haemochromatosis can be caused by pathogenic variants in the other genes (called non-HFE haemochromatosis). Juvenile haemochromatosis corresponds classically to type 2, which can be subdivided into type 2A, related to mutations in the hemojuvelin gene, and type 2B, related to mutations in the hepcidin gene. Furthermore, mutations in the TFR2 and SLC40A1 genes can be associated to haemochromatosis (more details below)[4].
The clinical diagnosis of iron overload is of course the starting point before treating and monitoring the patient. Early diagnosis and treatment are essential for improving survival and for a better quality of life[5]. The present review focuses on new information on classification, pathophysiology, and therapeutic recommendations.
EPIDEMIOLOGY
The HEIRS study evaluated, among other aspects, the prevalence of the HFE p.Cys282Tyr and p.His63Asp genetic alterations in a sample with 100000 adults during a period of 5 years in the United States and Canada. Among the obtained results, 299 subjects were homozygous for p.Cys282Tyr, and the estimated prevalence of p.Cys282Tyr homozygous was of 0.44% in white non-Hispanic subjects, 0.11% in native and American indigenous, 0.027% in Hispanic, 0.014% in Black, 0.012% in Pacific Island descendants and 0.000039% in Asiatic[6] subjects.
A review that selected 27 studies, totalling 6302 samples of subjects of European countries, showed the average prevalence of 0.4% for p.Cys282Tyr homozygotes and 9.2% for p.Cys282Tyr heterozygotes[7]. A cohort study with 22 centres across England, Scotland, and Wales in UK Biobank, including 451243 participants of European descent, identified 2890 (0.6%) individuals with p.Cys282Tyr homozygous genotype. The authors diagnosed haemochromatosis in 21.7% (95% confidence interval 19.5%-24.1%, 281/1294) of men and 9.8% (8.4%-11.2%, 156/1596) of women. Since p.C282Y-associated iron overload is preventable and treatable provided intervention is early, their findings justify reexamination of options for expanded early case ascertainment and screening[8]. Another study in blood donors in Brazil found 2.1% for the HFE 282Tyr allelic frequencies[9].
SYSTEMIC IRON REGULATION
Plasma iron finds its source in enterocytes and macrophages. It circulates, bound to transferrin, its iron transporter that can link up to two atoms of ferric iron (Fe3+). Transferrin-bound iron binds to transferrin receptor 1 on the plasma membrane of most cells, and forms a complex that is endocytosed. In the acidic environment of the endosome, ferric iron is reduced to ferrous iron (Fe2+) through the activity of a ferrireductase ( STEAP3). Ferrous iron is, then, released from the endosome to the cytosol via DMT1, and forms a labile iron pool. Iron leaves the cell through the activity of ferroportin, which is the only known protein to ensure cellular iron export into the plasma. Ferroportin export activity is regulated by the circulating hormone called hepcidin[10-13]. Hepcidin is a peptide essentially liberated by the hepatocytes[14-16]. The ferroportin-hepcidin binding at the level of the cell membrane induces the internalization, ubiquitination and degradation of intracellular ferroportin so that plasmatic levels of hepcidin strongly affect plasma iron concentration[17]. Low levels of hepcidin increase iron export from the enterocytes and macrophages, leading in turn to increased plasma iron concentration and transferrin saturation (TS) (Figure 2).
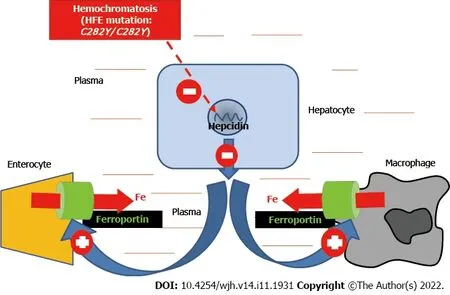
Figure 1 Mechanism of iron overload in HFE-related hemochromatosis. The C282Y/C282Y mutations (homozygosity for C282Y) lead to decreased synthesis of the iron hormone hepcidin, which in turn causes an increased activity of the iron export protein ferroportin both at the digestive and splenic levels. The result is increased plasma iron leading to organ iron overload.
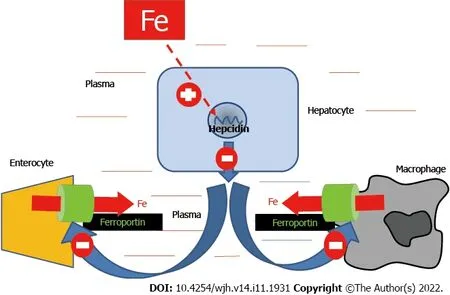
Figure 2 Schematic representation of systemic iron regulation. Physiologically, increased plasma iron leads to an increased synthesis of the iron hormone hepcidin, causing in turn decreased activity of the iron export protein Ferroportin both at the digestive and splenic levels, which leads to compensatory decreased plasma iron. The reverse mechanism occurs in case of physiological iron deficiency. Please note that, in haemochromatosis, the body behaves as if it was chronically iron deficient.
The adequate content of body iron requires the maintenance of plasma iron concentration within normal limits (12-25 μM) and the regulation of TS. Normal TS is between 20% and 45%, allowing adequate iron delivery to the cells[18]. In mammals, plasma iron binds to transferrin that is synthetized by the hepatocytes and, once released in the plasma, receives two atoms of ferric iron by an active process involving ferroxidase enzymes. When TS increases, non-transferrin bound iron may appear in the plasma and can lead to cell toxicity. The body is not capable of increasing iron excretion, even in case of iron excess. This holds true for genetic iron overload related to increased intestinal iron absorption, as well as for secondary iron overload that can be caused by repeated blood transfusions in the setting especially of chronic haemolytic anaemias, and various other haematological situations[19-24].
DIAGNOSIS
The diagnostic approach to haemochromatosis has become a noninvasive one, meaning that liver biopsy is no more needed. Indeed, haemochromatosis can be diagnosed on the sole combination of clinical, laboratory and imaging data.
Clinical features
Haemochromatosis can be asymptomatic for many years, and the lack of symptoms usually persists until adulthood, > 30 years old (and often > 40 in men and > 50 in women) in HFE-related haemochromatosis. In non-HFE haemochromatosis, the symptoms can appear around 20-30 years old. In general, the symptoms are diverse, which explains the frequent and harmful diagnosis delay[25-27].
Among the most common symptoms are fatigue and joint pain[28]. The dermatological signs are mainly melanoderma (dark pigmentation of the skin), but can also include skin dryness and nails alterations (and paradoxically koilonychia, a classical symptom of iron deficiency anaemia). The main liver symptoms are hepatomegaly and slight transaminase increase, contrasting with well-preserved liver functioning. Haemochromatosis can cause diabetes, hypogonadism or hypopituitarism[29]. It is of utmost importance to have in mind that HFE-haemochromatosis is only present in Caucasian populations or descents, and that non-HFE haemochromatosis, although much rarer, can be observed in many ethnic groups.
Laboratory tests
The most common diagn ostic biochemical tests consist of the following plasma parameters: iron, transferrin saturation (TS - determined from plasma transferrin concentration rather than from total iron binding capacity) and serum ferritin (SF). Increased TS is the earliest biochemical abnormality in haemochromatosis, reflecting increased iron absorption. It is > 45% (often > 60% in men and > 50% in women) and should be confirmed by a second assay. SF (> 300 μg/L in men and postmenopausal women, and > 200 μg/L in premenopausal women) can be raised in the inflammatory process, the metabolic syndrome (especially with diabetes), alcohol consumption and liver injury[30,31].
Genetic testing
Genetic testing is indicated whenever the patient has confirmed high levels of TS, provided other mechanisms than body iron excess have been ruled out (especially hypotransferrinemia due to hepatocellular failure, nephrotic syndrome or malnutrition). Haemochromatosis should not be seen as a simple monogenic disease, but as the complex result of the environment interaction, lifestyle and genetic factors that have not yet been fully identified. In case of HFE p.Cys282Tyr homozygosity, it is widely accepted that this genetic profile forms the necessary basis for the development of body iron excess[32]. Concerning the profile of compound heterozygosity p.Cys282Tyr and p.His63Asp, it can only predispose to mild iron overload and the physician should be careful when informing the patient, because alluding to haemochromatosis can cause unnecessary anxiety to the patient and its family[33,34].
When genetic testing for HFE provides a negative result, further genetic explorations, related to other genes involved in iron metabolism and hepcidin synthesis, can be conducted, requiring expert laboratories. Non-HFE haemochromatosis is less influenced by cofactors and characterized by a more severe and homogeneous clinical condition appearing at a younger age. Modern approaches, based on next generation sequencing (NGS), widely expand the possibilities of diagnosing these rare entities, but, at the same time, raise challenges for interpreting the results. NGS requires expert centres, either public or private, and its cost remains high but tend to decrease over time[35].
It should be kept in mind that, for most clinical practice worldwide, screening of HJV, HAMP, TFR2 and SLC40A1, and even of HFE, through direct sequencing is not widely available. Treatment is usually not dependent on molecular diagnosis[36-39]. It is therefore important to remember that, in this setting of difficult access to genetic identification, patients with a clinical diagnosis of haemochromatosis should not wait for the result of a DNA test before starting treatment.
Imaging tests
Magnetic resonance imaging (MRI) can be useful to assess and quantify body iron overload, especially in the liver, without forgetting to evaluate also the iron status of the spleen (the contrast between major liver iron excess and absence of spleen iron overload being highly suggestive of hepcidin deficiency). Laboratory examinations together with MRI have now largely replaced liver biopsy[40,20-22].
THERAPEUTIC RECOMMENDATIONS
The standard treatment for haemochromatosis remains phlebotomy (or therapeutic bleeding). This treatment has been shown to be effective and safe and has contributed to the reduction of morbidity and mortality in patients with haemochromatosis[41]. With each phlebotomy of 500 mL blood, approximate 250 mg iron are extracted and subsequently mobilized in a compensatory process from the organs where it had accumulated (especially the liver). Repeated phlebotomies result in the total removal of excess iron from the body. The therapeutic schedule must be individually adapted to each patient, and should take into account the patient’s levels of ferritin (according to the local reference values), age, gender and comorbidities. Recent studies have observed a beneficial effect in early and sustained treatment of patients with excess iron, even when iron overload was mild and/or SF only mildly elevated[32,42].
Table 1 shows two treatment phases: initial or intensive (induction), and the maintenance phase. Haemochromatosis patients under venesection therapy should never stop watching their iron parameters since the natural trend of increased iron absorption persists opening the risk of progressive iron excess reconstitution. Oral iron chelation is the commonly recommended treatment for iron overload related to chronic anaemia requiring regular blood transfusions. However, iron chelators may also be used as an alternative, or adjuvant, form of treatment in rare cases of haemochromatosis in which phlebotomies are contraindicated, not feasible due to problems in venous access, or if efficacy may not be not sufficiently achieved with phlebotomies alone in case of massive iron excess[43].
In the future, hepcidin-based treatments could potentially become an adjunct treatment to phlebotomy in the intensive phase or a substitute in the maintenance phase. The interest of restoring hepicidin levels is, of course, based on the fact that hepcidin deficiency is the mechanism accounting for the development of iron overload in patients with haemochromatosis[44].
EVOLUTION OF HAEMOCHROMATOSIS NOMENCLATURE
A working group of the International Society for the Study of Iron in Biology and Medicine (BIOIRON Society) proposed a new classification for haemochromatosis. The recent advances of pathophysiology and molecular basis of iron metabolism have highlighted that haemochromatosis is caused by mutations in at least five genes, resulting in insufficient hepcidin production or, rarely, resistance to hepcidin action. All these different data have led to a disease classification based on different molecular subtypes, mainly reflecting successive gene discoveries. When analysing the name of the disease, we can see the relation of something circulating in the blood haemo-) being responsible for skin and organ damage and pigmentation (-chromatosis). The work of recognizing excess iron as the aetiology of organ toxicity took several decades, and was attributable to Joseph Sheldon in 1935, who was also the first to suggest the genetic origin of the metabolic defect. Over time, it became evident that the genetic basis of haemochromatosis was more heterogeneous than initially thought, and several variants in other iron-controlling genes were progressively associated with the disorder. Unlike in the past, fully expressed and potentially lethal haemochromatosis with the full-blown picture associating liver cirrhosis, diabetes, endocrine dysfunction, and heart failure is rarely seen in current clinical practice. The novel classification aims to be practical whenever a detailed molecular characterization of haemochromatosis is not available[45].
Previous classification of haemochromatosis
Table 2 shows the previous classification of haemochromatosis. Most cases of haemochromatosis are caused by homozygous HFE p.Cys282Tyr genotype (type 1 haemochromatosis). The HFE gene is located on chromosome 6p21, encodes the haemochromatosis protein (HFE) which plays, through a not yet fully elucidated mechanism, a role in hepcidin regulation. As previously mentioned, the main symptoms are arthropathy, skin hyperpigmentation, liver damage, diabetes, endocrine dysfunctions, cardiomyopathy and hypogonadism. Haemochromatosis can also be caused, but much more rarely, by changes in other genes than HFE. These rare cases of haemochromatosis can be due to pathogenic variants in other genes, corresponding to non-HFE haemochromatosis. There were four entities: juvenile haemochromatosis (JH) or type 2 haemochromatosis, subdivided into two forms: Type 2A JH, caused by mutations in the HJV gene on chromosome 1q21, and type 2B JH, caused by mutations in the HAMP gene on chromosome 19q13. Type 2A genetic changes are involved in hepcidin synthesis, and are related to the BMP co-receptor. It has an early onset, in subjects younger than 30 years, and corresponds to severe forms of haemochromatosis. Type 2B haemochromatosis is related to a genetic defect of the HAMP gene, which encodes hepcidin. The main signs and symptoms are hypogonadism and cardiomyopathy. Haemochromatosis types 3 and 4 are caused by mutations in the TFR2 and SLC40A1 genes on chromosomes 7q22 and 2q32. Type 4 haemochromatosis, due to SLC40A1 mutations, is divided into 4A and 4B and has autosomal dominant inheritance. In type 4A, also named ferroportin disease, there is an alteration of ferroportin export activity leading to massive iron overload in the spleen, whereas TS is not elevated. Type 4B haemochromatosis is related to a gain of function process leading to ferroportin resistance to hepcidin and to clinical phenotype very close to that of type I haemochromatosis[46,47].
New classification of haemochromatosis proposed by an international expert working group
This working group proposed to de-emphasize the use of the molecular subtype criteria in favour of a classification better related to clinical issues. The group included both clinicians and basic scientists during a meeting in Heidelberg, Germany. The main ideas showing the need for changing the nomenclature were as follows: (1) Poor applicability in clinical practice; (2) Need for complex cooperation between geneticists, bioinformaticians and clinicians for resolving the most difficult cases, to determine the pathogenic nature or not of many variants; (3) Former type 4A haemochromatosis represents an iron overload syndrome strongly and clinically distinct from haemochromatosis (due to a different pathogenesis); (4) Former type 3 can correspond to JH; (5) Former type 3 haemochromatosis can be observed at an older age than JH[45]; and finally (6) Former type 4B, which corresponds to a hepcidin-refractory syndrome shares a similar phenotype to hepcidin-deficiency-related forms of haemochromatosis. Table 3 presents this new classification.
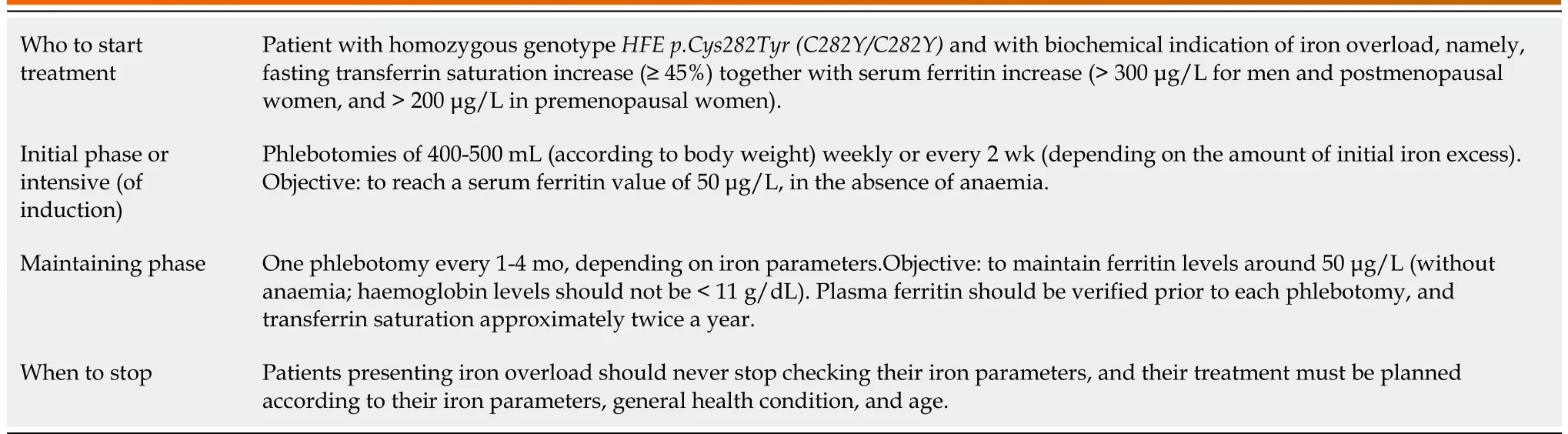
Table 1 Review about therapeutic recommendations
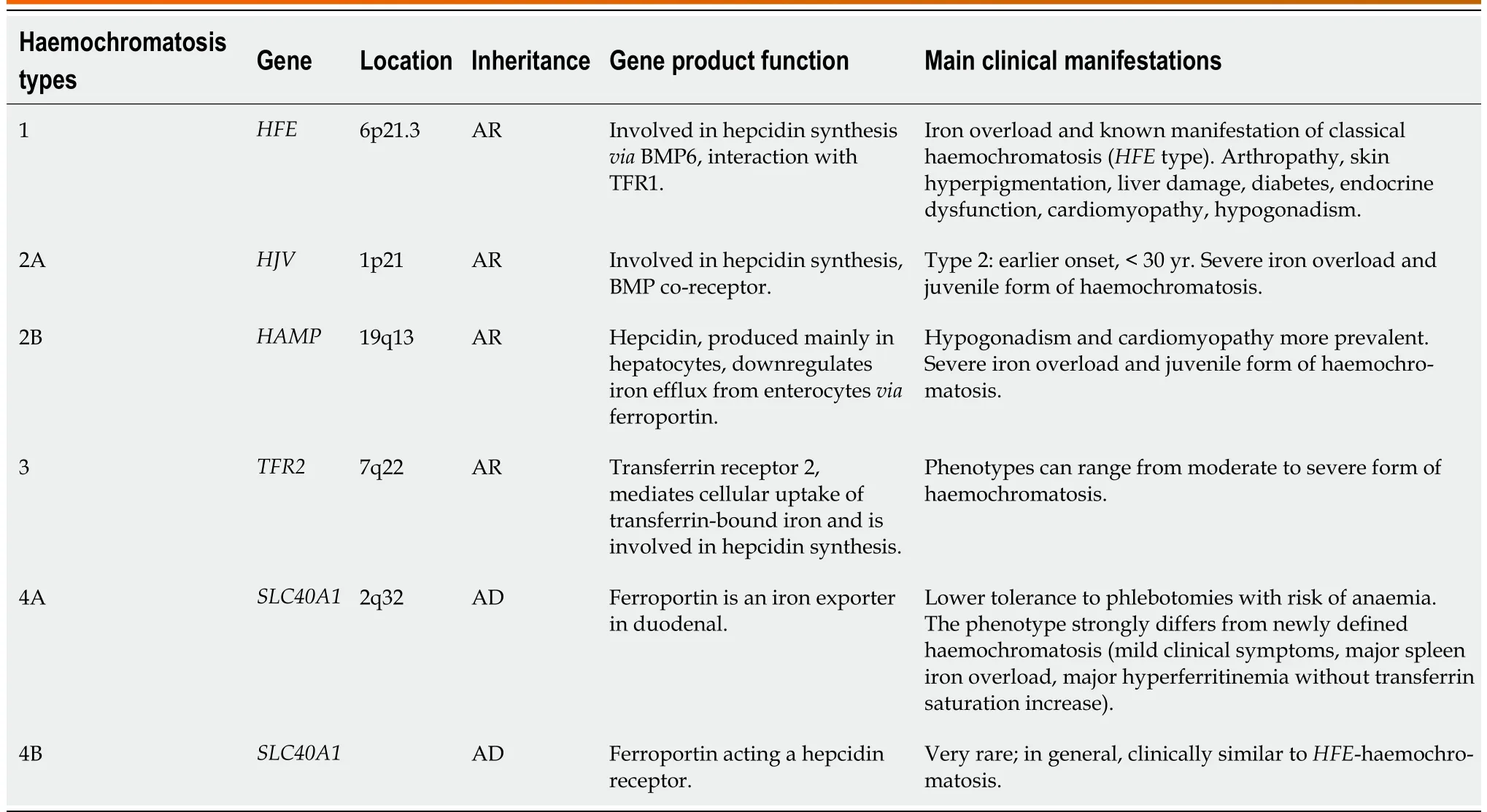
Table 2 Previous classification of haemochromatosis
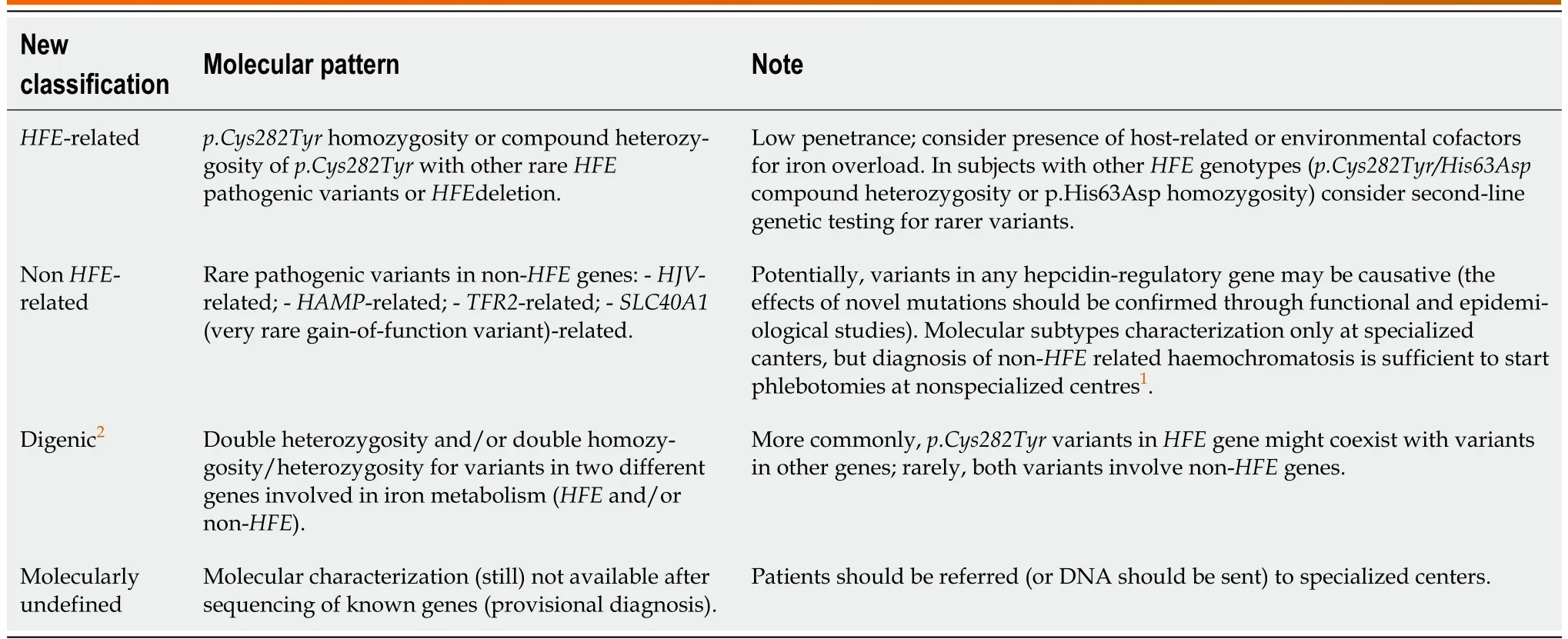
Table 3 New classification of haemochromatosis proposed by the working group
Rigorously speaking, the term haemochromatosis should now be reserved for a unique genetic clinicopathological condition characterized by increased TS, iron overload in the liver (but not in the spleen), prevalent involvement of periportal hepatocytes with iron spared Kupffer cells, and signs and/or symptoms associated with iron overload. Therefore, the term haemochromatosis should no longer be applied to all the previous subtypes. Finally, the panellists agreed that the definition of haemochromatosis should also include the absence of haematological signs of a primary/predominant red blood cell disorder, such as anaemia or reticulocytosis. In summary, as stated by the panellists, the novel classification proposed is based on a pathophysiological cornerstone (hepcidin deficiency) and a distinct clinical/biochemical phenotype. It recognizes the difficulties of a complete molecular characterization and has the potential of being easily shareable between practicing physicians and referral centres. Avoiding any ambiguity is essential for clear and effective communication that will facilitate proper diagnosis and treatment of haemochromatosis and was the main incentive for a real nom-enclature review[48].
CONCLUSION
It is strongly proposed to adopt, from now on, this new and more relevant classification of haemochromatosis that can be easily shared between practicing doctors and reference canters and will contribute to facilitate the diagnosis and therefore to improve the therapeutic management of haemochromatosis patients.
FOOTNOTES
Author contributions: Alvarenga AM, Brissot P, and Santos PC have contributed equally to this work.
Conflict-of-interest statement: All authors report no relevant conflict of interest for this article.
Open-Access: This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin: Brazil
ORCID number: Paulo Caleb Junior Lima Santos 0000-0002-8297-0793.
S-Editor: Wu YXJ
L-Editor: Kerr C
P-Editor: Wu YXJ
 World Journal of Hepatology2022年11期
World Journal of Hepatology2022年11期
- World Journal of Hepatology的其它文章
- Multiple hepatic infarctions secondary to diabetic ketoacidosis: Acase report
- Elevated calprotectin levels are associated with mortality in patients with acute decompensation of liver cirrhosis
- Liver test abnormalities in asymptomatic and mild COVID-19 patients and their association with viral shedding time
- Current status of disparity in liver disease
- Current management of liver diseases and the role of multidisciplinary approach