
Estimation of lung cancer burden in Australia, the Philippines, and Singapore: an evaluation of disability adjusted life years
2017-02-27 05:54:20SumanMorampudiNehaDasArunGowdaAnandPatilPhamaxAnalyticResourcesPvtLtdBengaluru560095India
Cancer Biology & Medicine 2017年1期
Suman Morampudi, Neha Das, Arun Gowda, Anand Patil Phamax Analytic Resources Pvt. Ltd., Bengaluru 560095, India
Estimation of lung cancer burden in Australia, the Philippines, and Singapore: an evaluation of disability adjusted life years
Suman Morampudi, Neha Das, Arun Gowda, Anand Patil Phamax Analytic Resources Pvt. Ltd., Bengaluru 560095, India
Objective: Lung cancer is one of the leading cancers and major causes of cancer mortality worldwide. The economic burden associated with the high mortality of lung cancer is high, which accounts for nearly $180 billion on a global scale in 2008. This paper aims to understand the economic burden of lung cancer in terms of disability adjusted life years (DALY) in Australia, the Philippines, and Singapore.
Lung cancer; DALY; YLD; YLL; burden of disease; DALY rate; discount rate
Introduction
Lung cancer is one of the leading cancers worldwide, with an estimated 1.8 million new cases recorded in 20121. According to the World Health Organization (WHO), lung cancer accounted for approximately 1.59 million cases of the 8.2 million cancer-related deaths reported in 2012; as such, lung cancer is one of the most significant causes of deaths worldwide1. Lung cancer is also the leading cancer among men and the third most common cancer type among women. The incidence rate of lung cancer worldwide varies between 0.8 and 53.5 cases per 100,000 population; the rate is high in Central Europe, Eastern Europe, and Eastern Asia and low in the Middle and West Africa1. Global estimates show that the age-standardized incidence rates of lung cancer are thehighest in Central and Eastern Europe and Eastern Asia, with 53.5 and 50.4 cases per 100,000 people, respectively1. Low age-standardized incidence rates of lung cancer among men (2.0 and 1.7 per 100,000, respectively) and women (1.1 and 0.8 per 100,000, respectively) were reported in Middle and West Africa1.
Epidemiologic studies suggest that lung cancer is the fifth most common cancer in Australia and the most common cause of cancer-attributable death among people aged 45-64 years2. In the Philippines, lung cancer is the most common cause of cancer-related mortality among men and the third most common cause of mortality and morbidity3. In Singapore, lung cancer is the second most common cancer in males and the third most common cancer in females, with reported lung cancer incidence rates of 16.2% in men and 7.7% among all cancer cases4.
Cancers account for the highest economic loss among the 15 leading causes of death worldwide. The total global economic loss incurred because of cancer burden was estimated to be $895 billion in 2008, which is 1.5% of the gross domestic product (GDP) worldwide5. Cancers of thelung, bronchus, and trachea conferred the major economic burden, accounting for nearly $180 billion on a global scale in 20085. The numbers are expected given that smokers die 15 years earlier than non-smokers on an average. The majority of lung cancer cases are reported in the middle aged and elderly population as a result of the increasing prevalence of smoking among young adults in the Asia-Pacific region6. Cancer symptoms require 10-30 years to develop; as such, the years of life lost or loss of productivity caused by cancer is a huge drain not only to the individual but also to the economy of these societies6. Despite epidemiologic studies suggesting that the incidence of lung cancer is relatively lower in the Asia-Pacific than that in the North America and Europe, recent studies show that the burden imposed by lung cancer on the health systems is enormous in the former. Furthermore, epidemiologic studies evaluating the true burden of lung cancer are insufficient in the Asia-Pacific region3-6.
This paper aims to understand the burden of lung cancer in three Asia-Pacific countries: Australia, Singapore, and the Philippines, and the burden of lung cancer is evaluated by understanding the economic loss caused by premature mortality and morbidity. To estimate the burden of lung cancer in Australia, the Philippines, and Singapore, we measure disability adjusted life year (DALY), which is calculated using years of life lost (YLL) and years lost due to disability (YLD). One DALY loss indicates the loss of 1 year of healthy life; thus, the total DALY in the entire population indicates the difference between the ideal healthy status without disease or disability and the current state. DALY is a sum of YLL caused by premature death and YLD. In simple terms, YLL represents the total number of lives lost prematurely because of early death caused by the disease. YLD represents the years lost due to disability and considers disability weightage, which reflects the severity of the disease on a scale of 0 (perfect health) to 1 (dead)7.
Methods
YLL and YLD were calculated using the formula developed by Lopez and Murray, as follows8:
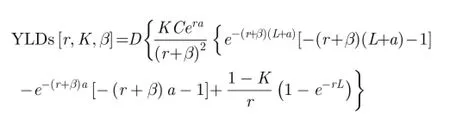
K=age weighting modulation factor; C=constant; r=discount rate; a=age of death; b=parameter from the age weighting function; L=standard expectation of life at age a.K=age weighting modulation factor; C=constant; r=discount rate; a=age of onset of disability; b=parameter from the age weighting function; L=duration of disability; D=disability weight.
The same formula is represented in the Global Burden of Disease (GBD) template provided by the WHO9. This formula uses the values defined in the WHO template, where the international standard discount rate is 0.03,K-values are 0 when no age weights are used and 1 when age weights are used; the standard age weights use a beta of 0.04 and a constant of 0.16588,10. However, theK-value was set to 0 because no age weights were used in the present study. The value ofDwas considered as 0.146 according to the WHO statistics and information system9. Although recent GBD studies did not apply age weights or discounts, the authors decided to use DALY calculations with discount rates; the US Panel on Cost-Effectiveness in Health and Medicine recommended the use of a 3% real discount rate to adjust both costs and health outcomes in economic analysis of health11. Moreover, numerous studies used discounts to calculate DALYs considering that the WHO reported timediscounted and age-weighted DALYs as their standards. Therefore, in the present study, the authors decided to compute DALYs with and without discounts so the results could be compared with those of other international studies.
Data
Population data for the three countries were sourced from the US Census Bureau12. The CI5plus database, which provides age- and sex-specific incidence data of cancer, was used to source diagnosed incident cases of lung cancer13. The CI5plus database, which was established by the International Agency for Research on Cancer, contains the updated annual incidence rates for all cancers up to 2007 in 118 selected populations worldwide13. The database is considered the gold-standard source for international cancer data and statistics because of its ability to provide validated annual incidence data, which can be used to compare accessible cancer incidence data among countries worldwide (Table 1)13. First, age- and sex-specific incidence rates for lung cancer from 2003 to 2007 were extracted. Regression analysis was then applied to the 5-year historical data obtained from CI5plus to calculate age- and sex-specific incidence ratesuntil 2015. In the absence of reliable evidence for change in trends in a specific age-group or in instances where researchers reported relatively stable trends, the incidence rate reported in the most recent year was kept constant throughout the forecast period. When regression analysis showed a decreasing/increasing trend that resulted in negative values or steep decline/incline in the incidence rate over the forecast period, the incidence rate reported/calculated in the most recent year was maintained constant throughout the forecast period.
We obtained incidence data from cancer registries and population-based studies published in peer-reviewed journals. The absolute number of lung cancer incident cases in each country were obtained by multiplying the age- and sex-specific incidence rates of lung cancer with the corresponding age and sex-specific population estimates. The calculated age-specific incident cases among men and women in each country were added to obtain the total diagnosed incident cases of lung cancer among men and women in each country.
Population-based studies or country-specific cancer registries were used to collect 5-year survival rates for lung cancer in each country (Table 2). A report by the Australian Institute of Health and Welfare Canberra was used to determine lung cancer survival rates for Australia.14For Singapore, lung cancer survival data for 1, 3, and 5 yearswere obtained from Cancer Survival data in Africa, Asia, the Caribbean, and Central America.15Similarly, lung cancer survival data for 1, 3, and 5 years in the Philippines were obtained from a journal article titled "Cancer and the Philippine Cancer Control Program.3Moreover, 2- and 4-year survival rates for Singapore and the Philippines were calculated by taking the average of the 1- and 3-year as well as 3- and 5-year data, respectively.
The 5-year survival rates obtained in the most recent year were kept constant throughout the forecast period because of lack of sufficient historical or contemporary data in each country. The survival rates for lung cancer in these countries were assumed not to have undergone any significant changes. The 5-year prevalent cases in each country were calculatedusing incident case data and relative survival data through a life-table method. The 1-year relative survival rate was applied to the total number of diagnosed incident cases for a specific year to obtain the expected number of cases that survived within that year. The 2-year relative survival rate was applied to the total number of diagnosed incident cases that were diagnosed 1-year ago to determine the expected number of cases that survived until year two. The same process was repeated to obtain 3-, 4-, and 5-year survival rates. Thus, the obtained 1- to 5-year prevalent cases in each year were added to obtain the 5-year prevalent cases of lung cancer in each country. The 5-year prevalence of lung cancer in each year was determined by dividing the calculated 5-year prevalent cases with the population estimates for that year. Considering that the 5-year survival rate varies by stages of lung cancer and data on the stage-specific survival rates of lung cancer for each year are not available from epidemiologic studies worldwide, researchers calculated the duration of disability based on incidence and prevalence rates to maintain uniform methodology across the countries16:
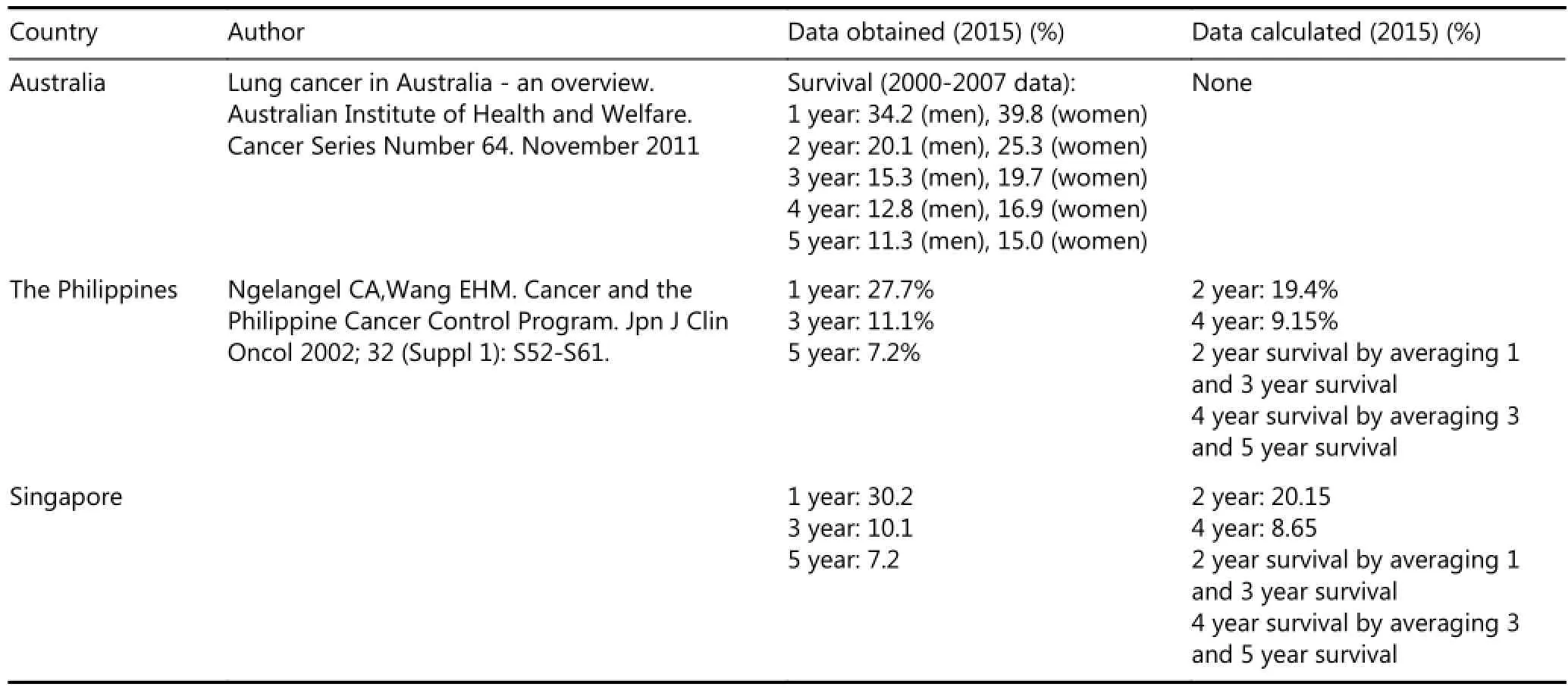
Table 2 Survival data
Prevalence=(Incidence Rate)×(Average Duration of Disease)
The duration of lung cancer in each year was obtained by dividing the 5-year prevalence in each year with the incidence rate for that year. Life expectancy is a critical aspect for calculation of YLDs; hence, constant life expectancy rates of 82.5 years at birth for women and 80 years at birth for men were maintained in each of the three countries17.
Researchers obtained the age- specific crude mortality rates for each country from country-specific sources because YLL calculation requires age-specific crude mortality cases (Table 3). Age-specific mortality rates were available from 2003 to 2013 for Australia18. Regression was then applied to the historical data to forecast the mortality cases of lung cancer in Australia during the forecast years. However, for Singapore and the Philippines, the studies provided overall mortality rates and not age-specific mortality rates for 2009-2013 and 2010, respectively19,20. To calculate the age-specific mortality rates in Singapore and the Philippines, researchers obtained the weights of age-specific mortality rates to the overall mortality rate in Australia. Researchers then applied these weights to the overall mortality rate in Singapore and the Philippines to obtain the age-specific mortality rates in these countries.
Results
The values of the burden of disease caused by lung cancer in 2015 in Australia, the Philippines, and Singapore were 91,695; 38,584; and 12,435 DALYs, respectively, as per a discount rate of 3% (Table 4). Australia presented the highest burden of disease caused by lung cancer. The DALY rate in Australia was 4.0 DALYs per 1,000 person-years, with the calculated burden of disease being the highest among people aged 45-79 years. Individuals aged 45-59, 60-69, and 70-79 years had 4.4, 12.6, and 18.5 DALYs per 1,000 person-years, respectively. This trend of increase in DALYs with increase in age from 45-79 years was also evident in the Philippines and Singapore. Although the Philippines presented the second highest calculated burden of lung cancer, the DALY rate was higher in Singapore (2.2 DALYs per 1,000 person-years) than that in the Philippines (0.4 DALYs per 1,000 person-years) (Figures 1-3).
When researchers calculated DALYs without a discount rate, the burden of disease increased substantially in these countries, with 117,438 DALYs in Australia, 50,977 in the Philippines, and 16,379 in Singapore (Table 5). Australia demonstrated the highest burden of disease caused by lung cancer even when the DALYs were calculated without using a discount rate. The DALY rate in Australia was 5.2 DALYs per 1,000 person-years, with the calculated burden of disease being the highest among people aged 70-79 years (21.8DALYs per 1,000 person-years). A similar trend was evident in the Philippines and Singapore, where people aged 70-79 years presented the highest calculated burden of lung cancer (the Philippines: 4.7 DALYs per 1,000 person-years and Singapore: 16.8 DALYs per 1,000 person-years) (Figures 1-3).
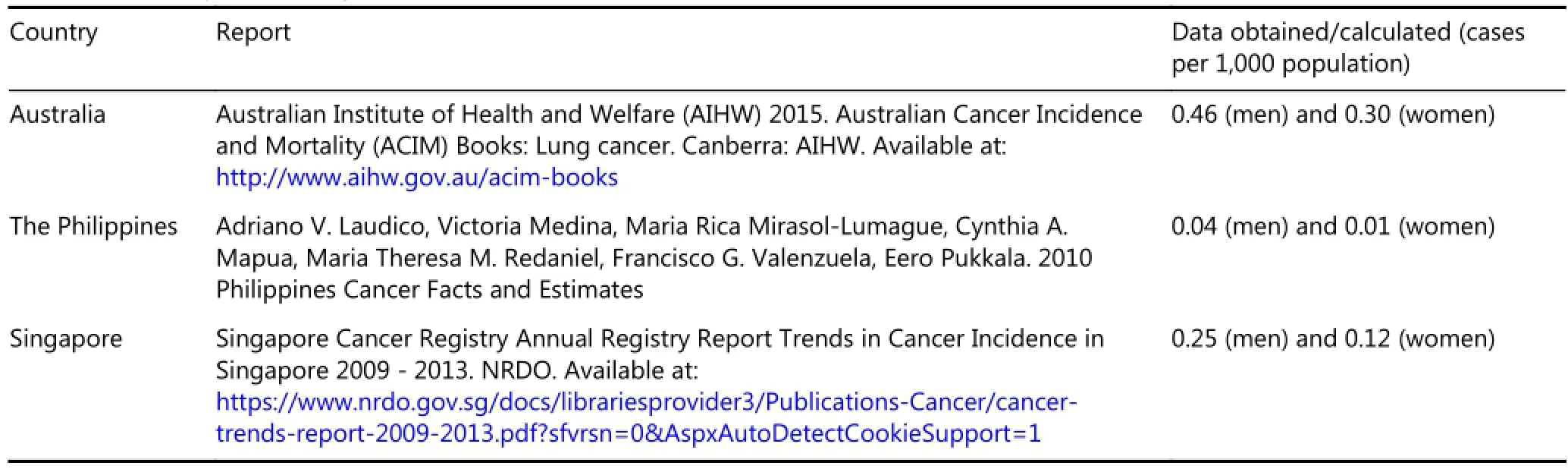
Table 3 Mortality rate of lung cancer
The high burden from lung cancers in each country was mainly due to mortality. Almost 98% of DALYs in Australia,96% in the Philippines, and 98% in Singapore were due to YLL.
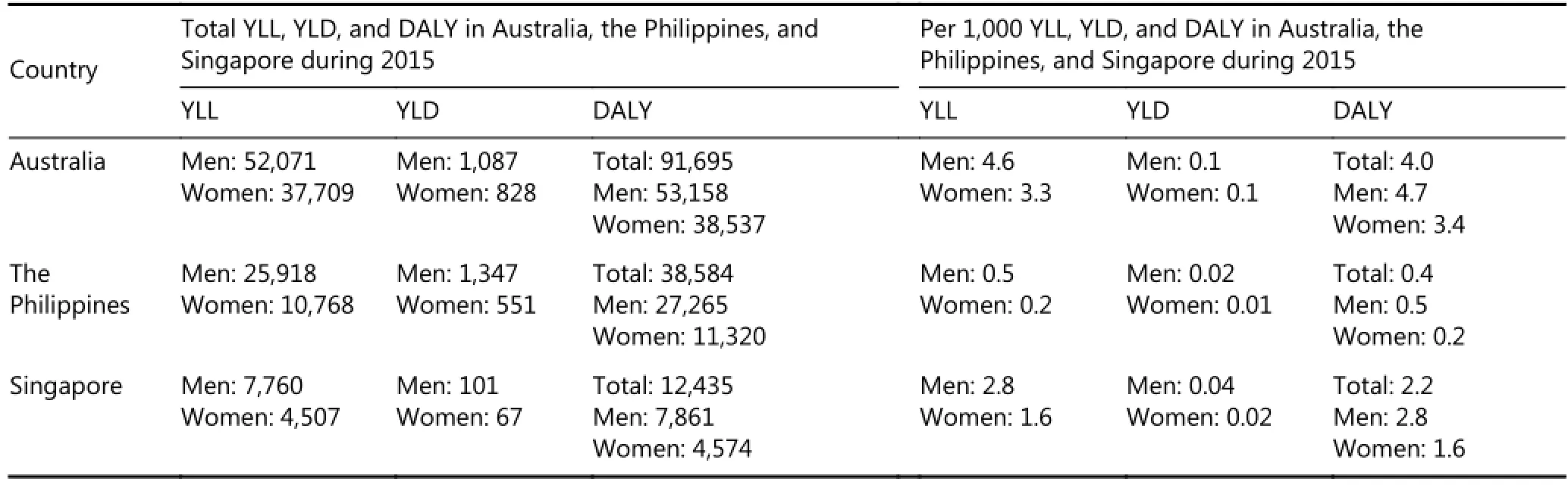
Table 4 DALY, YLL, and YLD calculated using a discount rate of 3%
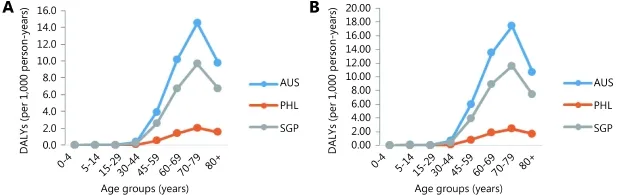
Figure 2 The age-specific rates of DALYs among women in Australia, the Philippines, and Singapore (2015) when a discount rate of 3% was used and when no discount rate was used. (A) Age-specific DALYs rate per 1,000 person-years among women in Australia, the Philippines and Singapore (using a discount rate of 3%). (B) Age-specific DALYs rate per 1,000 person-years among women in Australia, the Philippines and Singapore (without using a discount rate).
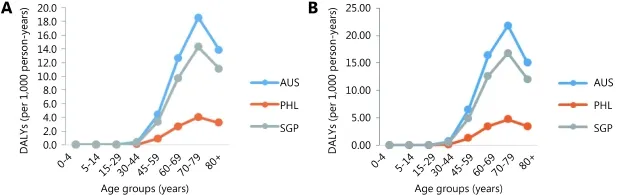
Figure 3 The age-specific rates of DALYs among men and women in Australia, the Philippines, and Singapore (2015) when a discount rate of 3% was used and when no discount rate was used. (A) Age-specific DALYs rate per 1,000 person-years among men and women in Australia, the Philippines and Singapore (using a discount rate of 3%). (B) Age-specific DALYs rate per 1,000 person-years among men and women in Australia, the Philippines and Singapore (without using a discount rate).
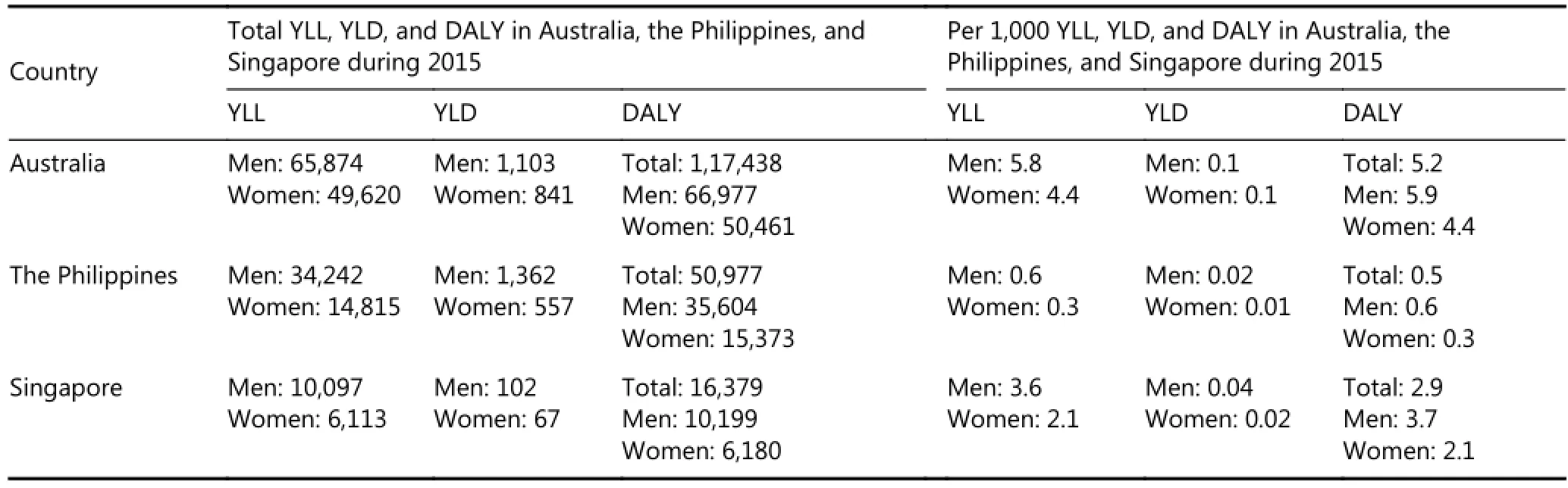
Table 5 DALY, YLL, and YLD calculated without using a discount rate
Gender distribution showed that both YLL and YLD were higher in males than those in females. The contribution of males to YLL, YLD, and DALY ranged from 52%-57% in Australia, 70%-72% in the Philippines, and 60%-62% in Singapore, respectively.
An age-wise distribution of DALYs showed that people aged 60-69 years in all three countries contributed to the highest number of DALYs (Table S1 to Table S6 in the supplementary materials, available with the full text of this article at www.cancerbiomed.org). However, people aged 60-69 years contributed almost 31% of all DALYs in their respective countries, with the highest per-capita DALYs detected in people aged 70-79 years in the three countries.
Discussion
Researchers of studies on burden of disease cannot always precisely predict the true burden posed by a disease, considering that analyses that involve estimates are often subject to errors. Different researchers may not arrive at the same conclusions because of their own distinctive and complex methods for estimating disease burden. Therefore, an intuitive and transparent methodology was adapted in the present study to present a comprehensible methodology for research peers. National level and country-specific estimates on lung cancer incidence, mortality, and survival were obtained to calculate the true burden of lung cancer in Australia, the Philippines, and Singapore.
Although the burden of disease studies no longer use discounts and age-weightage, DALYs were calculated with and without discount rates to compare findings with country-specific burden of disease studies. According to the Australian Institute of Health and Welfare (AIHW), lung cancer was predicted to be the leading cause of burden of disease due to cancer among men and the second highest burden of disease among women in Australia during 201221. The total number of people diagnosed with lung cancer in Australia in 2012 was 11,280 cases, which include 6,620 males and 4,650 females21. During the same period, the estimated number of deaths from lung cancer were 8,410 cases, whichinclude 5,070 males and 3,340 females21.
The AIHW study showed that the burden of lung cancer in 2012 was 57,300 DALYs among men (19% of the total cancer burden) and 43,400 DALYs among women (17% of the total cancer burden among women), with a discount rate of 3%21. The present study showed that the burden of lung cancer was 53,158 DALYs in men and 38,537 DALYs in women, with a discount rate of 3%. Although the DALYs calculated by the research team are lower than the AIHW results, the differences are minimal and can be attributed to the use of the Australian specific life expectancy tables and disability weights and not to the WHO standards22. In addition, the AIHW study used population estimates from the Australian Bureau of Statistics, whereas the present research group used census data from the International Database of the United States Census Bureau. Furthermore, the differences in estimates may be due to regression analysis of the historical incidence and mortality data22.
When the DALYs were calculated without discount rates, the results considerably differed from the AIHW estimates, with the burden of lung cancer increasing to 66,977 DALYs in men and 50,461 DALYs in women in 2015. Although a difference in the DALY estimates was expected by the researcher group when no discount rate was used, the difference was remarkable. The causes of this difference remain unclear but could be partially attributed to the use of different population estimates and increasing trend of lung cancer incidence. Hence, the results implicate a significant disability caused by lung cancer among Australians.
Similarly, in Singapore and the Philippines, lung cancer is the commonly diagnosed and one of the leading causes of mortality among cancers in the ASEAN region. Singapore presents high age standardized (ASR) mortality due to lung cancer in this region, whereas the Philippines has a low agestandardized mortality rate among males and females combined6,23. According to the Singapore burden of diseases study (SBoD), cardiovascular diseases and cancers accounted for 40% of the total DALYs in 2010, of which 80% was due to mortality23. In Singapore, lung cancer contributed to 3.4% or 13,589 of the total DALYs (total DALY 399,675) in 201023. The findings from this study, which was conducted using a methodology similar to that used in the SBoD study, showed that lung cancer burden in Singapore was 12,435 DALYs. Moreover, the SBoD study showed that lung cancer accounted for 4.4% (9,252) and 2.4% (4,546) of the total 210,267 DALYs among males and 189,408 DALYs among females, respectively23. The present study found these values to be 7,861 and 4,574 DALYs among males and females, respectively. The difference in DALYs between the SBoD study in 2010 and those calculated by the researchers with a discount rate of 3% could be due to the use of Singaporespecific standard life expectancy tables in the SBoD study with increasing burden of lung cancer in Singapore24. Although no other studies have evaluated the burden of lung cancer in Singapore without using a discount rate, the present study found the burden to be 16,379 DALYs.
In the Philippines, as per a previous study that estimated lung cancer burden without using a discount rate, the estimated DALYs were 104,442 in 200825. However, the value was found to be 50,977 DALYs in this study, which is less than half of the DALYs reported in a 2008 Philippines study. Although both studies were conducted using the same methodology, the differences in DALYs can be attributed to the use of DISMOD II for assessment of disease epidemiology rather than obtaining estimates from the CI5plus database as well as to the assumptions and projections made by the authors. When a discount rate of 3% was used, the DALYs decreased further to 38,584 in 2015. The Philippines is the only country that showed significant differences in DALYs among the three countries of interest. Furthermore, the majority of DALYs in these countries were caused by mortality. This finding is consistent with the findings from previous studies, where 99% of DALYs was due to YLL in the Philippines and 93% of DALYs were due to YLL in Singapore23,25. The high incidence and mortality rates and poor survival rates for lung cancer among older individuals can be attributed to the strong effect of YLLs among DALYs in these countries.
Furthermore, the incidence, prevalence and mortality estimates made by the researchers are approximately similar to the projections made by GLOBOCAN26,27. Notwithstanding the positives that arise out of this study, limitations were also present. Although the estimated DALYs are believed to reflect the actual lung cancer burden in these countries, the burden may considerably vary if varying prevalence of causal agents or other risk factors are considered when estimating DALYs.
Conclusions
Despite the major achievements in the field of oncology, the prognosis for lung cancer remains extremely poor and has only improved marginally over the decades. Data from the past three decades in Australia show that the 5-year survival rates marginally increased between 1982 and 2010. The 5-year survival was 8% for males and 10% for females during 1982-1987 and 13% for males and 17% for females during 2006-2010. At the same time, morbidity due to lung cancer has increased over the years. The number of hospitalizationsfor lung cancer in Australia increased by 29% between 2000-2001 and 2008-200914,18,21. This trend is not limited to just Australia but is widely evident worldwide6,19,25,28.
Considering the high mortality rates caused by lung cancer worldwide, appropriate strategies must be developed to manage the disease. Cancer burden can be controlled and reduced by identifying and developing strategies that focus on prevention, early diagnosis, and treatment. Initiatives such as the WHO Framework Convention on Tobacco Control can significantly reduce economic loss due to lung cancer29. Tobacco, alcohol, obesity, unhealthy diet, physical inactivity, pollution, radiation, and infections are considered the main cancer risk factors worldwide30. Given that smoking tobacco is one of the leading risk factors accounting for almost 70% of lung cancer deaths globally, the main focus should be on preventive strategies that reduce smoking. Studies have shown that interventions reduce the prevalence of smoking and have proven to be cost-effective. Although numerous countries have already formulated and enforced regulations to restrict tobacco usage, most health care systems have failed in giving priority to smoking interventions6.
In the Philippines, the Lung Cancer Control Program utilizes primary and tertiary prevention at special medical centers and rehabilitation activities to control smoking. Awareness messages have been spread through collaboration with Department of Education, Culture, and Sports and Bureau of Secondary Education in schools31. Regulations such as labeling and advertising on cigarette packs are being encouraged. Smoking is prohibited in workplaces, schools, gyms, parks, hospitals, elevators, and stairwells of all buildings, buses and bus depots, restaurants, and government facilities3,31. Singapore implemented the legislation of smokefree public places in 1970 and was the first Asian country to ban tobacco advertisements in 1971. Warnings for smokers have also been implemented. As a result, the country has one of the lowest smoking rates worldwide32. Currently, Singapore is implementing the point of sale display ban to reduce exposure of non-smokers to smoke. Moreover, the National Cancer Center of Singapore currently treats 60%-70% of all subsidized patients and 50% of all cancer patients in the country28. The Cancer Council Australia develops cancer control policy resources, including prevention, early detection, clinical practice (treatment), and supportive care. Regulations such as reducing the affordability of tobacco products, strengthening mass media campaigns, eliminating advertising and promotion, and promoting smoke free zones are being encouraged33. To add to its many initiatives, Australia became the first nation to implement the plain packaging of tobacco products in 2012. Since the implementation of the plain packaging act, tobacco consumption decreased by 2.9% in a quarter and 12.2% over the year, at 2 years after the inception of the legislation34.
All these attempts at improving lung cancer management are substantial. However, more collaborative efforts encompassing all aspects of chronic disease management are needed. These efforts include advocacy, providing information for policy, health promotion, surveillance, prevention, and management. Additional information is presented in Tables S1 to S18 in the supplementary document.
Conflict of interest statement
No potential conflicts of interest are disclosed.
1.Ferlay J, Ervik M, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: 2013; IARC Cancer Base No. 11: [Internet] 2013. Available from: http://globocan.iarc.fr. [Last accessed on 2016 May 21].
2.AIHW. Australian burden of disease study: Fatal burden of disease 2010. Australian Burden of Disease Study Series No. 1. Cat. No. BOD 1. Canberra: AIHW.
3.Corazon A. Ngelangel and Wang EHM. Cancer and the philippine cancer control program. Jpn J Clini Oncol. 2002; 32: S52-S61.
4.NUCI. Lung cancer. 2012. Available from: http://www.ncis.com.sg/cancer-information/types-ofcancer/thoracic-lung.html. [Last accessed on 2016 Apr 17].
5.ACS. The global economic cost of cancer. 2010; 1st ed. American Cancer Society; 2010. Available from: http://www.cancer.org/acs/groups/content/@internationalaffairs/do cuments/document/acspc-026203.pdf. [Last accessed on 2016 May 24].
6.Bilano VL, Borja MP, Cruz EL, Tan AG, Mortera LL, Reganit PF. Smoking-attributable burden of lung cancer in the philippines. Tob Control. 2015; 24: 263-8.
7.WHO. Health statistics and information systems, metrics: Disability-adjusted life year (daly). 2015. Available from: http://www.who.int/healthinfo/global_burden_disease/metrics_dal y/en/. [Last accessed on 2016 May 24]
8.Lopez CJ, Murray AD. The global burden of disease. A comprehensive assessment of mortality and disability for diseases, injuries and risk factors in 1990 and projected to 2020. Cambridge: Harvard University Press, 1996.
9.WHO. Health statistics and information systems, national tools. 2015. Available from: http://www.who.int/healthinfo/global_burden_disease/tools_national/en/. [Last accessed on 2016 May 24]
10.Fox-Rushby JA, Hanson K. Calculating and presenting disability adjusted life years (dalys) in cost-effectiveness analysis. Health Policy Plan. 2001; 16: 326-31.
11.Gold M. Panel on cost-effectiveness in health and medicine. Medical care 1996; 34:DS197-9.
12.United States Census Bureau. Population estimates. 2015. Available from: https://www.census.gov/popest/data/. [Last accessed on 2016 April 25]
13.Ferlay J BF, Steliarova-Foucher E, Forman D. Cancer incidence in five continents. CancerBase No. 9.: Lyon: International Agency for Research on Cancer, 2014.
14.AIHW. Lung cancer in australia: An overview 2011. 2011; Cat. no. CAN 58; 206pp. Australian Institute of Health and Welfare Canberra.
15.IARC. Comparison of 1-, 3- and 5- year- absolute and relative survival and 5 year age standardised relative survival by site. IARC. Cancer care survival in Asia, Africa, the Caribbean and Central America. 2015. Available from: http://survcan.iarc.fr/survivalstatsicd10.php?ICD10=C33-34&tableTable3&soumisson=subm. [Last accessed on 2016 Feb 16]
16.CDC. Principles of epidemiology in public health practice. An introduction to applied epidemiology and biostatistics: Centers for Disease Control and Prevention; 2012.
17.Murray CJ. Quantifying the burden of disease: The technical basis for disability-adjusted life years. Bull World Health Organ. 1994; 72: 429-45.
18.AIHW. Australian cancer incidence and mortality (acim) books: Lung Cancer 2015. Available from: http://www.aihw.gov.au/acimbooks/. [Last accessed on 2016 May 19]
19.Lee Hin Peng CL, Chow Khuan Yew, Zheng Huili, William Ho. Singapore cancer registry annual registry report trends in cancer incidence in singapore 2009–2013. 2014; NRDO. Available from: https://www.nrdo.gov.sg/docs/librariesprovider3/Publications-Cancer/cancer-trends-report-2009-2013.pdf?sfvrsn=0&AspxAutDetectCookieSupport=1. [Last accessed on 2016 Feb 16]
20.Adriano V. Laudico VM, Maria Rica Mirasol-Lumague, Cynthia A. Mapua, Maria Theresa M. Redaniel, Francisco G. Valenzuela Eero Pukkala. Philippines cancer facts and estimates. 2010;
21.AIHW. Cancer in australia: An overview 2012; Cancer series no. 74 2012, Australian Institute of Health and Welfare & Australasian Association of Cancer Registries Canberra.
22.Begg STV, Barker B, Stevenson C, Stanley L, Lopez AD. The burden of disease and injury in australia 2003. 2007; Cat. no. PHE 82. Canberra: AIHW. Available from: http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=64424 59747. [Last accessed on 2016 Feb 16]
23.Singapore MoH. Singapore burden of disease study 2010. 2014. Available from: https://www.moh.gov.sg/content/dam/moh_web/Publications/Rep orts/2014/Singapore%20Burden%20of%20Disease%20Study%202 010%20Report_v3.pdf. [Last accessed on 2016 May 4]
24.Phua HP, Chua AV, Ma S, Heng D, Chew SK. Singapore's burden of disease and injury 2004. Singapore Med J. 2009; 50: 468-78.
25.Kimman M, Norman R, Jan S, Kingston D, Woodward M. The burden of cancer in member countries of the association of southeast Asian nations (ASEAN). Asian Pac J Cancer Prev. 2012; 13: 411-20.
26.Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015; 136:E359-86.
27.Bray F, Ren JS, Masuyer E, Ferlay J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int J Cancer. 2013; 132: 1133-45.
28.Teo MC, Soo KC. Cancer trends and incidences in Singapore. Jpn J Clin Oncol 2013; 43:219-24.
29.WHO. Who framework convention on tobacco control. 2016;
30.CDC. What are the risk factors for lung cancer? Available from: http://www.cdc.gov/cancer/lung/basic_info/risk_factors.htm. [Last accessed on 2016 May 25].
31.ANS. Philippines. Available from: http://www.nosmoke.org/goingsmokefree.php?id=622. [Last accessed on 2016 May 16].
32.Singapore MoH. Fact sheet: Tobacco control. Available from: https://www.moh.gov.sg/content/dam/moh_web/PressRoom/Highl ights/2014/COS%202014/Details%20on%20Tobacco%20Control.p df. [Last accessed on 2016 May 21].
33.Grogan P. National cancer control policy: Tobacco control. Available from: http://wiki.cancer.org.au/policy/Tobacco_control. [Last accessed on 2016 May 22].
34.Australian Government. Tobacco plain packaging act 2011. 2013; 148. Available from: https://www.legislation.gov.au/Details/C2013C00190. [Last accessed on 2016 May 26]
Cite this article as: Morampudi S, Das N, Gowda A, Patil A. Estimation of lung cancer burden in Australia, the Philippines, and Singapore: an evaluation of disability adjusted life years. Cancer Biol Med. 2017; 14: 74-82. doi: 10.20892/j.issn.2095-3941.2016.0030
Suman Morampudi
E-mail: suman.morampudi@fs-researchcenter.com Received March 18, 2016; accepted May 25, 2016. Available at www.cancerbiomed.org
Copyright ? 2017 by Cancer Biology & Medicine
Methods:The years of life lost (YLL) and years lost due to disability (YLD) were calculated using the formula developed by Murray and Lopez in 1996 as part of a comprehensive assessment of mortality and disability for diseases, injuries and risk factors in 1990 and projected to 2020. The same formula is represented in the Global Burden of Disease template provided by the World Health Organization. Appropriate assumptions were made when data were unavailable and projections were performed using regression analysis to obtain data for 2015.
Results:The total DALYs due to lung cancer in Australia, the Philippines, and Singapore were 91,695, 38,584, and 12,435, respectively, and the corresponding DALY rates per a population of 1,000 were 4.0, 0.4, and 2.2, respectively, with a discount rate of 3%. When researchers calculated DALYs without the discount rate, the burden of disease increased substantially; the DALYs were 117,438 in Australia, 50,977 in the Philippines, and 16,379 in Singapore. Overall, YLL or premature death accounted for more than 95% of DALYs in these countries.
Conclusions:Strategies for prevention, early diagnosis, and prompt treatment must be devised for diseases where the major burden is due to mortality.
 Cancer Biology & Medicine2017年1期
Cancer Biology & Medicine2017年1期
- Cancer Biology & Medicine的其它文章
- Erratum to Bcl-2 expression is a poor predictor for hepatocellular carcinoma prognosis of andropause-age patients
- Metformin prevents hormonal and metabolic disturbances and 1,2-dimethylhydrazine-induced colon carcinogenesis in non-diabetic rats
- Truth telling for patients with esophageal squamous cell carcinoma in Henan, China
- Roles of Rap1 signaling in tumor cell migration and invasion
- A pilot study of radiologic measures of abdominal adiposity: weighty contributors to early pancreatic carcinogenesis worth evaluating?
- Association of genotypes of rs671 within ALDH2 with risk for gastric cardia adenocarcinoma in the Chinese Han population in high- and low-incidence areas