
Safety of different acupuncture manipulations for posterior circulation ischemia with vertigo
2016-12-01 09:23:31YanWenChaoZhangXiaofengZhaoShizheDengSiHeLinghuiHuangGuangTianZhihongMengDepartmentofAcupunctureandMoxibustionFirstTeachingHospitalofTianjinUniversityofTraditionalChineseMedicineTianjinChina2InstituteofAcupuncturean
中國神經(jīng)再生研究(英文版) 2016年8期
Yan Wen, Chao Zhang, Xiao-feng Zhao, Shi-zhe Deng Si He Ling-hui Huang, Guang Tian Zhi-hong Meng Department of Acupuncture and Moxibustion, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, China2 Institute of Acupuncture and Moxibustion, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, China Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu Province, China
Safety of different acupuncture manipulations for posterior circulation ischemia with vertigo
Yan Wen1,#, Chao Zhang1,#, Xiao-feng Zhao2,#, Shi-zhe Deng1, Si He1, Ling-hui Huang3, Guang Tian1, Zhi-hong Meng1,*
1 Department of Acupuncture and Moxibustion, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, China
2 Institute of Acupuncture and Moxibustion, First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, China
3 Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu Province, China
How to cite this article: Wen Y, Zhang C, Zhao XF, Deng SZ, He S, Huang LH, Tian G, Meng ZH (2016) Safety of different acupuncture manipulations for posterior circulation ischemia with vertigo. Neural Regen Res 11(8)∶1267-1273.
Funding: This study was supported by the National Basic Research Program of China (973 Program), No. 2010CB530506.
Zhi-hong Meng, Ph.D.,
tjmzh86@163.com.
#These authors contributed
equally to this study.
orcid:
0000-0002-8470-2696
(Zhi-hong Meng)
Accepted: 2016-07-19
Graphical Abstract
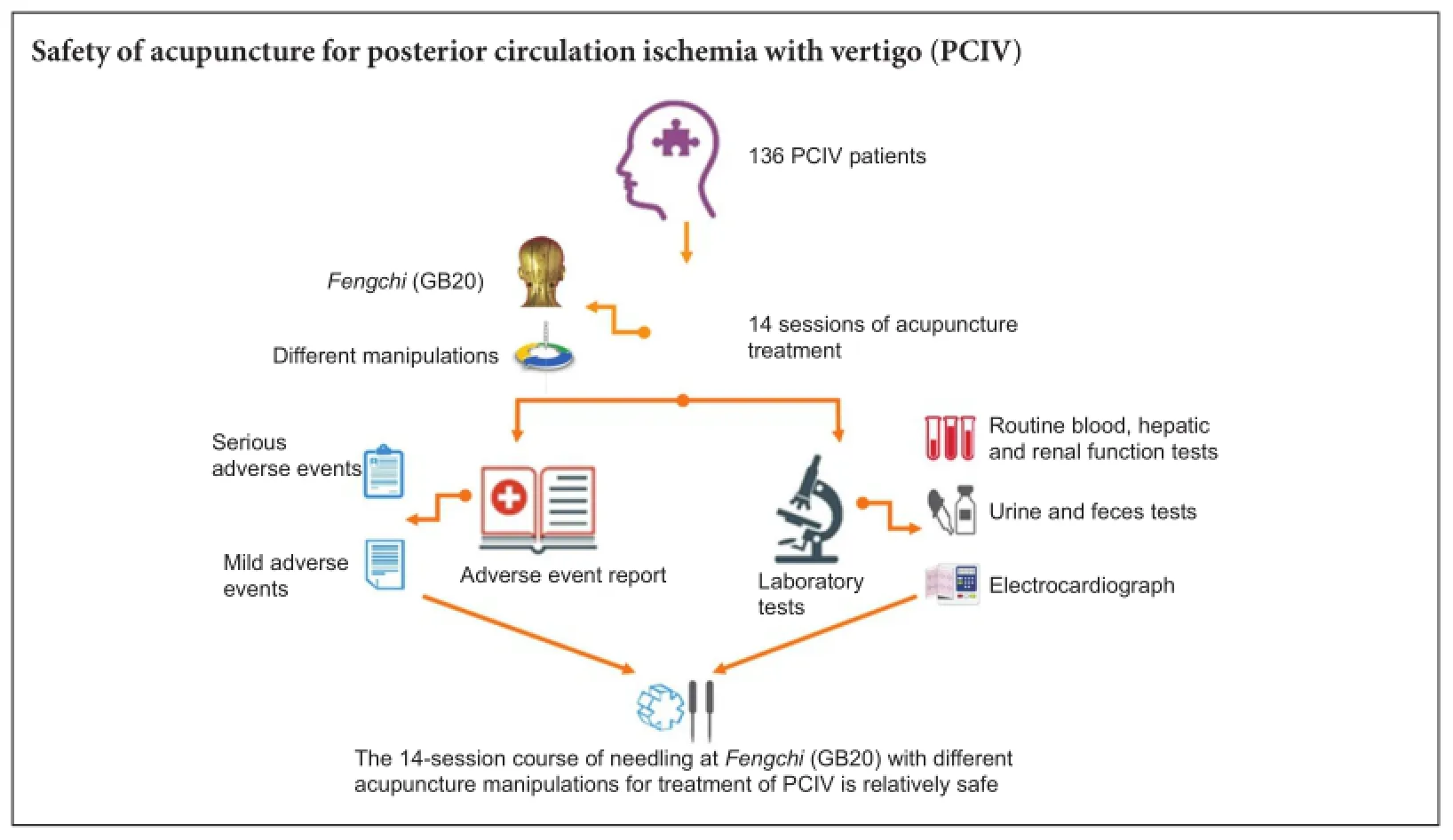
Acupuncture at Fengchi (GB20) in the posterior neck improves vertigo. However, subarachnoid hemorrhage and spinal epidural hematoma have been reported to occur after acupuncture in the posterior neck. Therefore, in the present study, we assessed the safety of acupuncture at Fengchi. Laboratory tests and adverse event reports were used to evaluate the safety of different acupuncture manipulations for the treatment of posterior circulation ischemia with vertigo. A total of 136 patients were randomly assigned to four groups. Verum acupuncture was conducted with different needle insertion directions (contralateral paropia or prominentia laryngea) and different needle twisting frequencies (60 or 120 times/minute) at Fengchi and matching acupoints (for example, Zhongwan [CV12], Qihai [CV6], Zusanli [ST36], and Fenglong [ST40]). The patients received 14 treatments over 3-4 weeks. Routine blood analysis, hepatic and renal function tests, urine and feces tests and electrocardiography were performed before the first treatment session and after the final session. Adverse events were recorded after every session. Of the 136 patients, 120 completed the study. There were no significant differences between pretreatment and posttreatment test results in any of the groups. Only five patients suffered from minor adverse events (needling pain, slight hematoma and transient chest tightness). No serious adverse events were found. Our results indicate that a 14-session course of needling at Fengchi is relatively safe for treating posterior circulation ischemia with vertigo.
nerve regeneration; posterior circulation ischemia; vertigo; acupuncture; direction; twisting frequency; Fengchi (GB20); adverse event; safety; neural regeneration
Introduction
Frequent symptoms of posterior circulation ischemia (PCI) include vertigo, nystagmus, coma and ataxia. Vertigo is the main symptom of PCI (Searls et al., 2012). Acupuncture treatment improves symptoms of vertigo resulting from PCI (Zhao et al., 1997). The Fengchi (GB20) acupoint is commonly used in the treatment of vertigo, and promotes blood flow.
Acupuncture has been used in China for thousands of years and its use is growing in many other countries suchas the USA, UK, Australia, Canada, Denmark and Norway (Hanssen et al., 2005; MacPherson et al., 2006; Xue et al., 2008; Zhang et al., 2012). The greater acceptance of acupuncture worldwide has led to increasing demands for evidence of its effectiveness and safety, important for both patients and acupuncture practitioners. Serious adverse events associated with acupuncture, including viral hepatitis, pneumothorax, and nerve injury, have been documented, mostly in case reports and retrospective surveys (Yamashita et al., 2001; Ernst and Sherman, 2003; Lao et al., 2003). However, these serious adverse events or complications have rarely been found in prospective studies addressing acupuncture safety, although mild and transient adverse events such as needling pain, bleeding or hematoma are common (White et al., 2001; Endres et al., 2004; MacPherson et al., 2004; Witt et al., 2009). Together, this evidence suggests that acupuncture is a relatively safe procedure.
The safety of acupuncture is an important issue and deserves careful attention. A recent systematic review of Chinese literature about acupuncture-related adverse events (Zhang et al., 2010) revealed that the acupoints most frequently involved in cases of subarachnoid hemorrhage and spinal epidural hematoma are located on the posterior neck, for example at Fengchi, the main acupoint in the present study. In addition to the acupoint location, needling manipulations such as the direction and depth of insertion (Lin et al., 2013) might also be associated with acupuncture-related adverse events. Therefore, in the present study, we used standard laboratory tests and adverse event reporting to evaluate the safety of needling at Fengchi as a treatment for PCI with vertigo (PCIV) using different acupuncture manipulations (direction and twisting frequency).
Subjects and Methods
Study design
We performed a randomized prospective controlled trial in patients with PCIV. This study was performed in the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine in China, which is known as the National Clinical Research Center of Acupuncture and Moxibustion, China. With the approval of the regional ethics review boards of Tianjin University of Traditional Chinese Medicine, 250 patients were screened between 1 February 2012 and 1 December 2013.
Subjects
Electronic bulletin boards and notices on printed recruitment posters were placed in the Outpatient Department at the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, China. Interested patients were referred to the study investigators, and screening evaluations were conducted by experienced clinicians. Patients were screened for participation if they fulfilled the following diagnostic criteria proposed by the World Health Organization (WHO Task Force on Stroke and other Cerebrovascular Disorders, 1989): (1) dizziness or vertigo; (2) vertebrobasilar insufficiency revealed by transcranial Doppler/magnetic resonance imaging; (3) major symptoms possibly accompanied by unsteadiness or ataxia; unilateral or bilateral visual, motor or sensory disturbances; double vision; dysarthria or swallowing impairment; acute impairment of consciousness or acute confusion.
Inclusion criteria: Male or female patients meeting all of the following criteria were considered for admission to the trial:
(1) Diagnosed with vertebrobasilar insufficiency; (2) aged between 40 and 75 years; (3) volunteered to undergo acupuncture treatment and able to cooperate with the inspection; (4) provided signed informed consent.
Exclusion criteria: Patients presenting with one of the following conditions were excluded from the trial:
(1) Cerebral hemorrhage and bulbar paralysis; (2) aural or ocular vertigo; (3) systolic blood pressure ≥ 180 mmHg and/ or diastolic blood pressure ≥ 120 mmHg; (4) Glasgow coma scale score of < 15 or Hasegawa’s dementia scale score of <27.5; (5) serious heart, liver or kidney disease; (6) critical illness requiring surgery; (7) pregnancy or lactation; (8) severe mental illness; (9) currently participating, or participated in the past 3 months, in other clinical research.
All patients who met the inclusion criteria were given ample time to decide whether they would participate in the study. All patients who wanted to enter the study signed the informed consent form. This trial was registered at the Chinese Clinical Trial Registry (ChiCTR-RTRCC-12002675) and performed according to the principles of the Declaration of Helsinki. The trial protocol was approved by the Medical Ethics Committee, Tianjin University of Traditional Chinese Medicine, China (approval No. TJUTCM-EC20110005). Figure 1 shows the study flow chart.
Randomization and group assignment
All subjects were randomly assigned to one of four verum acupuncture groups according to a randomization list generated in Excel 2003 and using numbered, opaque, sealed envelopes. Groups and main acupuncture points are defined in Figure 2. The outcome assessors and statistician were blinded to the experimental grouping.
Acupuncture administration
We used sterile disposable stainless steel needles (length: 40 mm, diameter: 0.25 mm; Hwatuo, Suzhou Medical Supplies Factory Co., Ltd., Suzhou, Jiangsu Province, China). Patients underwent 14 treatment sessions over 3-4 weeks. Each session lasted 20 minutes. Fengchi (inferior to the occipital bone, in the depression between the origins of the sternocleidomastoid and trapezius muscles) was selected as the main acupoint, and matching acupoints were added based on individualized pattern diagnoses: Zhongwan (CV12, on the anterior midline, 4 cun above the umbilicus); Qihai (CV6, on the anterior midline, 1.5 cun below the umbilicus); Zusanli (ST36, three cun directly below Dubi (ST35) and one finger-breadth lateral to the anterior border of the tibia); Fenglong (ST40, one finger-breadth lateral to Tiaokou (ST38) and at the midpoint of the line joining Dubi and thetip of the external malleolus); Taixi (KI3, in the depression between the tip of the medial malleolus and the Achilles tendon); Zhaohai (KI6, in the depression directly below the tip of the medial malleolus); Neiguan (PC6, on the line joining Daling (PC7) and Quze (PC3), between the tendons of palmaris longus and flexor carpi radialis, 2 cun above the transverse crease of the wrist); Laogong (PC8, on the radial aspect of the third metacarpal bone, at the tip of the middle finger when a fist is made and the finger is flexed). The angle, depth, and manipulation of matching acupoints conformed to typical prescriptions. Needling manipulations were performed manually by one experienced acupuncturist who had been practicing for more than 20 years.
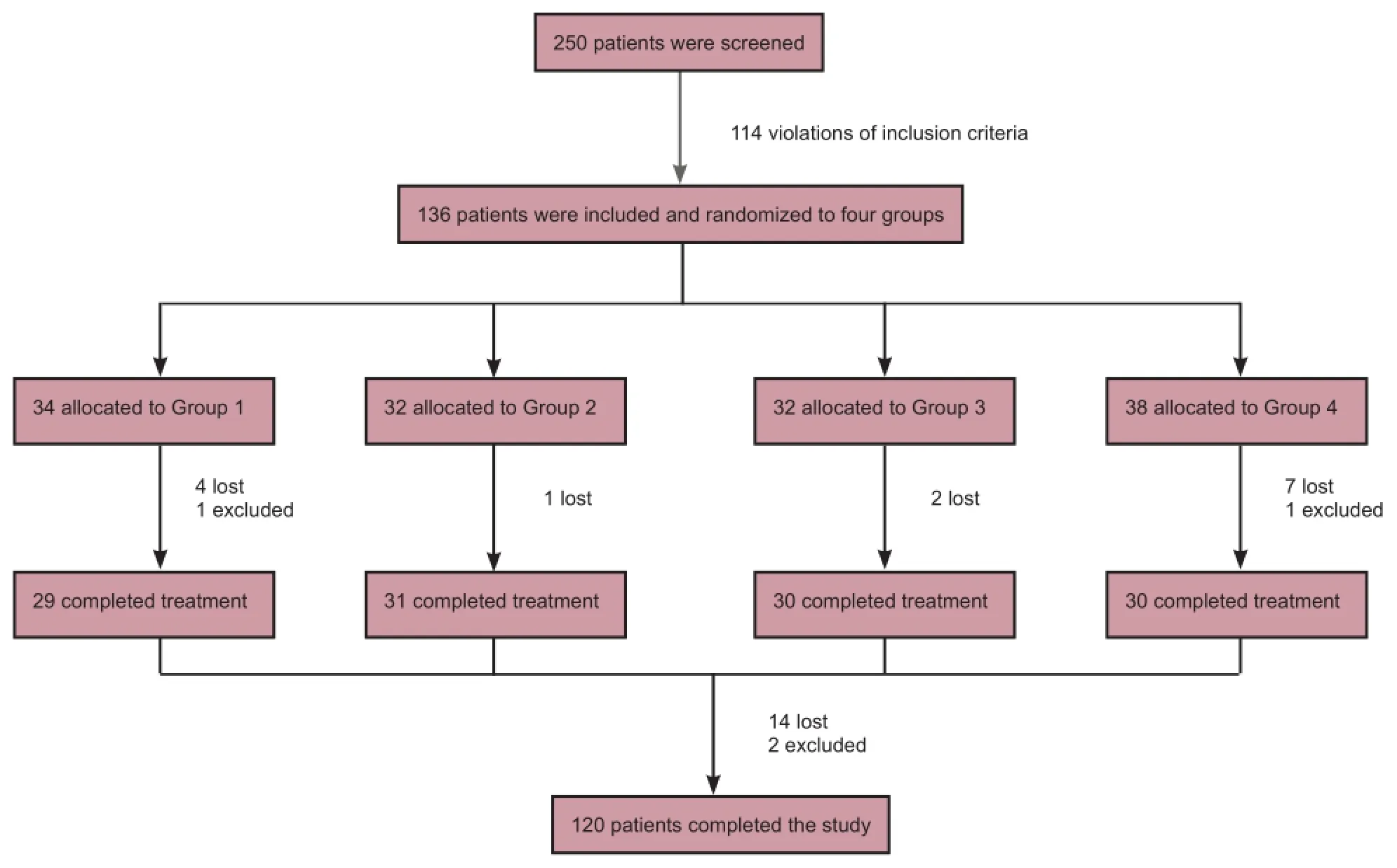
Figure 1 Flow chart of the study.

Figure 2 Main needling point and manipulations in the four groups. GB20: Fengchi acupoint.
Needling at the main acupoint Fengchi was performed with the patient sitting. For needle retention, the patient lay prone. The needle was manually inserted deeply (0.5-0.8 cun) in either the contralateral paropia or prominentia laryngea direction, and twisted 60 or 120 times for 1 minute. After Deqi (a sensation of numbness, distension, or electrical tingling at the needling site, which might radiate along the corresponding meridian), the needles were retained in place for 20 minutes.
Outcome measures
Laboratory tests were performed before the first acupuncture session and after the final session. Adverse events, including pain, hematoma, perforation, bleeding, fainting, local infection, abscess, or breakage or retention of the needle after treatment, were recorded after every session.
The laboratory tests comprised routine blood analysis, hepatic and renal function measurement, urine and feces tests and electrocardiography (ECG).
Routine blood analysis included hemoglobin level and counts of leukocytes, erythrocytes, neutrophilic granulocytes and lymphocytes.
Hepatic and renal function tests comprised measurement of carbamide, creatinine, total protein, albumin, globulin, alanine aminotransferase and aspartate transaminase.
Urine tests included measurement of excreted protein and glucose, and counts of leucocytes and erythrocytes. The fecal occult blood test was also conducted.
Twelve-lead ECGs were performed with patients in the supine position. Heart rate and rhythm, durations of P-wave, QRS interval and QT(c) interval, and QRS axis were evaluated. ECG variables were analyzed with standard ECG nomenclature and definitions.
Blood, urine and feces samples were collected at 8:00 a.m. on the day before the first treatment and the day after the final treatment. Normal values for all laboratory tests were provided by the Clinical Laboratory in the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, China.

Table 1 Demographic and clinical characteristics at baseline

Table 2 Routine blood test results
Sample size
We estimated the sample size with the formula used in previous relevant literature. We planned to enroll 144 participants (36 per group), allowing for a 15% dropout rate.
Statistical analysis
All data, expressed as the mean ± SD, were statistically analyzed using SPSS v19.0 (IBM, Armonk, NY, USA). Data were analyzed by study personnel and a statistician blinded to experimental grouping. Analysis of covariance and paired t-test were used to analyze measurement data. The chi-square test was used for enumerated data.
Results
Quantitative analysis of patients
Two hundred and fifty patients were screened. Of these, 136 with PCIV met the inclusion criteria, gave signed consent, and were randomly assigned to four verum acupuncture groups. Of those enrolled, 14 were lost during the treatment course, because they had difficulties in keeping to the schedule, and two were excluded. Altogether, 120 patients completed the study (29 in group 1, 31 in group 2, 30 in group 3 and 30 in group 4). The demographic characteristics for participants are shown in Table 1. There were no significant differences between the groups in mean age, body mass index, age of vertigo onset, or commonly used drugs (all P >0.05); a significant difference was found in sex ratio between the groups (P < 0.05).
Routine blood analysis
Neutrophil percentage in group 4 and lymphocyte percentage in group 1 were significantly greater after acupuncture treatment than before (both P < 0.05). All other within-group comparisons were non-significant (P > 0.05). All pretreatment and posttreatment blood test results were in the normal range (Table 2).
Hepatic and renal function
Aspartate transaminase levels were statistically greater after treatment than before in groups 3 and 4 (P < 0.05). For albumin, the pretreatment value was significantly higher than the posttreatment value in group 4 only (P < 0.05). Alanine aminotransferase level in group 1 was significantly higher after treatment than before (P < 0.05). All other within-group comparisons were nonsignificant (P > 0.05). Despite these differences, all measures of hepatic and renal function in thefour groups were in the normal range before and after treatment (Table 3).

Table 3 Hepatic and renal function test results

Table 4 Results of urine and feces tests and electrocardiograph
Urine and feces tests and ECG
No significant differences were found in urine and feces tests or ECG after treatment compared to baseline (P > 0.05). Moreover, the number of patients with values outside the normal rage did not increase after 14 treatments (Table 4).
Adverse events
No serious adverse events were reported. Several mild adverse events occurred during the study. One patient in group 4 had a mild hematoma at the acupuncture site shortly after treatment. No patients were terminated from the study because of pain, but two patients (one in group 1 and one in group 4) did complain that acupuncture was very painful and one patient in group 3 felt mild pain at the acupuncture site more than one hour after treatment. One patient in group 2 suffered from chest tightness from the supine position, but this symptom disappeared when the patient changed position to sitting.
Discussion
Our results demonstrate that the protocol of needling at Fengchi in two different directions (contralateral paropia or prominentia laryngea) and twisting frequencies (60 or 120 per minute) is relatively safe for patients with PCIV. This will be valuable in the design of randomized clinical trials addressing the role of acupuncture in PCIV or other diseases.
The laboratory tests we chose to investigate acupuncture safety (blood analysis, hepatic and renal function measurements, urine and feces tests, and ECG) are commonly used as screening tests to investigate drug safety. Changes in certain biochemical indexes are considered sensitive markers for certain diseases. For example, elevated albumin excretion and abnormal levels of proteinuria are indicative of chronic kidney disease (Keane and Eknoyan, 1999; Levey et al.,2003), and leukocyte and neutrophil numbers are markers of the inflammatory reaction. Dufour et al. (2000) indicated that aspartate transaminase, alanine aminotransferase, total protein, and albumin should be used to evaluate patients with known or suspected liver disease; of these, alanine aminotransferase is the most important test for identifying acute and chronic hepatic disease. Liver diseases such as hepatitis and bacterial and viral infections have been repeatedly associated with acupuncture (MacPherson et al., 2004; Karmochkine et al., 2006; Nguyen et al., 2007; Ernst et al., 2011). There has been some reduction in the number of reports addressing hepatic disease and infection resulting from acupuncture in recent years (White, 2004); however, as acupuncture gains an increasingly important role in today’s multidisciplinary clinics, its complications, although infrequent, cannot be overlooked.
To the best of our knowledge, the present study is the first to use laboratory tests to explore the influence of acupuncture on hematological and biochemical indexes. The lack of difference between pre- and posttreatment values in the present study provides measurable evidence for the clinical safety of acupuncture and may be useful in pursuing further studies on its safety using different manipulations.
We found no serious adverse events in the present study. This result is consistent with several prospective surveys of acupuncture safety from the UK (MacPherson et al., 2001; White et al., 2001). Two other surveys, conducted in Germany-one comprising more than 2 million consecutive acupuncture treatments in 229,230 patients (Witt et al., 2009) and the other more than 760,000 acupuncture treatments (Melchart et al., 2004)-reported only a few serious adverse events; these included pneumothorax and nerve damage. Serious acupuncture-related adverse events may be classified into two categories: traumatic and infectious. The majority of the traumatic injuries could have been avoided if the acupuncturists had better anatomical knowledge and received professional training (Peuker and Gr?nemeyer, 2001). In our study, needling manipulations were performed by an experienced acupuncturist who had been practicing for more than 20 years. Furthermore, the acupuncturist received professional training before our trial to ensure accuracy of needle manipulation. The qualified acupuncturist plays an important role in avoiding serious adverse events, and acupuncture can be considered safe in the hands of competent practitioners (Vincent, 2001).
Another common type of adverse event is infection. Hepatitis, human immunodeficiency virus and subacute bacterial endocarditis represent the three most serious infectious complications resulting from acupuncture (Ernst and White, 1997). Infections result primarily from poor aseptic procedure and insufficient knowledge of practitioners, who often disinfect reusable acupuncture needles with alcohol instead of sterilizing them (Zhang et al., 2010). Our study used sterile disposable stainless steel needles. To avoid cross-contamination, each patient had their own needles and the acupuncturist adopted strict sterilization procedures. The use of disposable sterile acupuncture needles is strongly recommended (World Health Organization, 1999) and is mandatory in some western countries, but may not be fully established in non-western countries, especially in rural areas (Sun et al., 1999; Sanchez et al., 2000; Shin et al., 2000). The use of disposable needles is important to ensure the safety of acupuncture. Based on the above, we propose that if acupuncture is used according to established safety rules and carefully at appropriate anatomic regions by a qualified acupuncturist, it is a relatively safe treatment method.
In contrast to serious complications, mild adverse reactions to acupuncture are common. However, despite previous literature showing a strong association between needling pain, slight hemorrhage and hematoma with acupuncture (Ernst and Sherman, 2003; Nguyen et al., 2007; Witt et al., 2009; Capili et al., 2010), few adverse events were observed in our study. Only five patients reported adverse events throughout the treatment period; of these, three experienced needling pain, one had a minor hematoma and one reported transient chest tightness. A previous study demonstrated that men and elderly individuals experienced most adverse events (Zhao et al., 2011). In the present study, the average age was 59.36 years and 70% of subjects were female; this, combined with the high tolerance for acupuncture treatment in China, may contribute to the low incidence of adverse events we observed.
Our study has several limitations. First, a relatively brief treatment period was chosen, so the study demonstrates that a 14-session acupuncture protocol is safe for people with PCIV, but longer durations of treatment should be investigated. The second limitation was the small sample size. We know that the best evidence of treatment safety is a largescale prospective study or meta-analysis. If the samples were larger, this would provide a better evaluation of acupuncture safety.
In summary, we used laboratory tests and adverse event reporting to assess the safety of different acupuncture manipulations in patients with PCIV. Laboratory data from 120 subjects showed no clinical differences between pre- and posttreatment values; no serious adverse events were associated with acupuncture and only five patients suffered any adverse events throughout the treatment period. Our data indicate that needling at Fengchi to treat PCIV, in different directions (towards the contralateral paropia or prominentia laryngea) and at different twisting frequencies (60 or 120 twists per minute) when conducted by a qualified acupuncturist, is relatively safe. Further research is needed to explore acupuncture safety under different conditions and for longer treatment periods.
Acknowledgments: We sincerely thank Acupuncture and Moxibustion Research Institute of Tianjin University of Traditional Chinese Medicine in China for offering the experimental areas and instruments.
Author contributions: ZHM and XFZ conceived the study and prepared the initial protocol. YW and CZ drafted the paper and participated in the study design. SZD, SH and LHH completed the study. GT analyzed the data. All authorsapproved the final version of the paper.
Conflicts of interest: None declared.
Plagiarism check: This paper was screened twice using Cross-Check to verify originality before publication.
Peer review: This paper was double-blinded and stringently reviewed by international expert reviewers.
References
Capili B, Anastasi JK, Geiger JN (2010) Adverse event reporting in acupuncture clinical trials focusing on pain. Clin J Pain 26:43-48.
Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB (2000) Diagnosis and monitoring of hepatic injury. I. Performance characteristics of laboratory tests. Clin Chem 46:2027-2049.
Endres HG, Molsberger A, Lungenhausen M, Trampisch HJ (2004) An internal standard for verifying the accuracy of serious adverse event reporting: the example of an acupuncture study of 190,924 patients. Eur J Med Res 9:545-551.
Ernst E, White A (1997) Life-threatening adverse reactions after acupuncture? A systematic review. Pain 71:123-126.
Ernst E, Sherman K (2003) Is acupuncture a risk factor for hepatitis? Systematic review of epidemiological studies. J Gastroenterol Hepatol 18:1231-1236.
Ernst E, Lee MS, Choi TY (2011) Acupuncture: does it alleviate pain and are there serious risks? A review of reviews. Pain 152:755-764.
Hanssen B, Grimsgaard S, Launs? L, F?nneb? V, Falkenberg T, Rasmussen NK (2005) Use of complementary and alternative medicine in the Scandinavian countries. Scand J Prim Health Care 23:57-62.
Karmochkine M, Carrat F, Dos Santos O, Cacoub P, Raguin G (2006) A case-control study of risk factors for hepatitis C infection in patients with unexplained routes of infection. J Viral Hepatitis 13:775-782.
Keane WF, Eknoyan G (1999) Proteinuria, albuminuria, risk, assessment, detection, elimination (PARADE): a position paper of the National Kidney Foundation. Am J Kidney Dis 33:1004-1010.
Lao L, Hamilton GR, Fu J, Berman BM (2003) Is acupuncture safe? A systematic review of case reports. Altern Ther Health Med 9:72-83.
Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, Hogg RJ, Perrone RD, Lau J, Eknoyan G (2003) National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med 139:137-147.
Lin JG, Chou PC, Chu HY (2013) An exploration of the needling depth in acupuncture: the safe needling depth and the needling depth of clinical efficacy. Evid Based Complement Alternat Med 2013:740508.
MacPherson H, Sinclair-Lian N, Thomas K (2006) Patients seeking care from acupuncture practitioners in the UK: a national survey. Complement Ther Med 14:20-30.
MacPherson H, Thomas K, Walters S, Fitter M (2001) The York acupuncture safety study: prospective survey of 34000 treatments by traditional acupuncturists. BMJ 323:486-487.
MacPherson H, Scullion A, Thomas K, Walters S (2004) Patient reports of adverse events associated with acupuncture treatment: a prospective national survey. Qual Saf Health Care 13:349-355.
Melchart D, Weidenhammer W, Streng A, Reitmayr S, Hoppe A, Ernst E, Linde K (2004) Prospective investigation of adverse effects of acupuncture in 97733 patients. Arch Intern Med 164:104-105.
Nguyen VT, McLaws ML, Dore GJ (2007) Highly endemic hepatitis B infection in rural Vietnam. J Gastroenterol Hepatol 22:2093-2100.
Peuker E, Gr?nemeyer D (2001) Rare but serious complications of acupuncture: traumatic lesions. Acupunct Med 19:103-108.
Sanchez JL, Sjogren MH, Callahan JD, Watts DM, Lucas C, Abdel-Hamid M, Constantine NT, Hyams KC, Hinostroza S, Figueroa-Barrios R, Cuthie JC (2000) Hepatitis C in Peru: risk factors for infection, potential iatrogenic transmission, and genotype distribution. Am J Trop Med Hyg 63:242-248.
Searls DE, Pazdera L, Korbel E, Vysata O, Caplan LR (2012) Symptoms and signs of posterior circulation ischemia in the new England medical center posterior circulation registry. Arch Neurol 69:346-351.
Shin HR, Kim JY, Ohno T, Cao K, Mizokami M, Risch H, Kim SR (2000) Prevalence and risk factors of hepatitis C virus infection among Koreans in rural area of Korea. Hepatol Res 17:185-196.
Sun CA, Chen HC, Lu CF, You SL, Mau YC, Ho MS, Lin SH, Chen CJ (1999) Transmission of hepatitis C virus in Taiwan: prevalence and risk factors based on a nationwide survey. J Med Virol 59:290-296.
Vincent C (2001) The safety of acupuncture. BMJ 323:467-468.
White A (2004) A cumulative review of the range and incidence of significant adverse events associated with acupuncture. Acupunct Med 22:122-133.
White A, Hayhoe S, Hart A, Ernst E (2001) Adverse events following acupuncture: prospective survey of 32 000 consultations with doctors and physiotherapists. BMJ 323:485-486.
WHO Task Force on Stroke and other Cerebrovascular Disorders (1989) Recommendations on stroke prevention, diagnosis, and therapy. Stroke 20:1407-1431.
Witt CM, Pach D, Brinkhaus B, Wruck K, Tag B, Mank S, Willich SN (2009) Safety of acupuncture: results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forsch Komplementmed 16:91-97.
World Health Organization (1999) Guidelines on Basic Training and Safety in Acupuncture.
Xue CC, Zhang AL, Lin V, Myers R, Polus B, Story DF (2008) Acupuncture, chiropractic and osteopathy use in Australia: a national population survey. BMC Public Health 8:105.
Yamashita H, Tsukayama H, White AR, Tanno Y, Sugishita C, Ernst E (2001) Systematic review of adverse events following acupuncture: the Japanese literature. Complement Ther Med 9:98-104.
Zhang J, Shang H, Gao X, Ernst E (2010) Acupuncture-related adverse events: a systematic review of the Chinese literature. Bull World Health Organ 88:915C-921C.
Zhang Y, Lao L, Chen H, Ceballos R (2012) Acupuncture use among american adults: what acupuncture practitioners can learn from national health interview survey 2007? Evid Based Complement Alternat Med 2012:710750.
Zhao HX, Wang WZ, Wang S, Zhou P (1997) Effect of acupuncture in patient with vertebrobasilar insufficiency, reports of 102 cases. Zhongguo Zhen Jiu 17:211-213.
Zhao L, Zhang FW, Li Y, Wu X, Zheng H, Cheng LH, Liang FR (2011) Adverse events associated with acupuncture: three multicentre randomized controlled trials of 1968 cases in China. Trials 12:87.
Copyedited by Slone-Murphy, Norman C, Yu J, Qiu Y, Li CH, Song LP, Zhao M
10.4103/1673-5374.189191
*Correspondence to:

- 中國神經(jīng)再生研究(英文版)的其它文章
- Secondary parkinsonism induced by hydrocephalus after subarachnoid and intraventricular hemorrhage
- Huangqi Guizhi Wuwu Decoction for treating diabetic peripheral neuropathy: a meta-analysis of 16 randomized controlled trials
- No synergism between bis(propyl)-cognitin and rasagiline on protecting dopaminergic neurons in Parkinson's disease mice
- Association between chromosomal aberration of COX8C and tethered spinal cord syndrome: arraybased comparative genomic hybridization analysis
- Rebuilding motor function of the spinal cord based on functional electrical stimulation
- Acellular allogeneic nerve grafting combined with bone marrow mesenchymal stem cell transplantation for the repair of long-segment sciatic nerve defects: biomechanics and validation of mathematical models