
Clinical Study of MELD System Direct Assessment theDegree of Hepatic Fibrosis for LT Patient
2010-01-25 05:01:00ZuoHuaiquanXiaDongQuanYiYanLuNanZengYongXuMingqingWangWentao
中國腫瘤外科雜志 2010年5期
Zuo Huai-quan, Xia Dong, Quan Yi, Yan Lu-Nan, Zeng Yong, Xu Ming-qing, Wang Wen-tao,
Yang Jia-ying, Wu Hong
1 Introduction
The Model for End-Stage Liver Disease (MELD) scoring system was proposed by Malinchoc in 2000 to predict the survival in patients undergoing transjugular intrahepatic portosystemic shunt[1]. Kamath et al[2]in 2001 verified the ability of this model to predict the prognosis of chronic liver disease, and with slight modifications of the original model, they developed the end-stage liver disease formula. This formula is believed to be more accurate and objective to predict the severity and the prognosis of chronic liver disease. Subsequently, MELD was used in donor liver allocation by UNOS[3-4]. However, there have been very few reports to validate objectively the correlation between the MELD score with the degree of hepatic fibrosis and cirrhosis.
Hepatic fibrosis and cirrhosis are a spectrum of pathological processes which go hand in hand together. Theoretically, the more the hepatic fibrosis, the less are the functional liver cells and the worse is the cirrhosis. The ability to quantitatively assess hepatic fibrosis and cirrhosis in an individual patient is of paramount importance in clinical practice. Currently there are a number of indirect methods to assess the degree of cirrhosis[5-6]such as serological index, quantitative liver function tests, and imaging techniques using ultrasonography, computed tomography and magnetic resonance. These indirect techniques still need to be validated with histopathological study of the liver.
Percutaneous needle biopsy of the liver has been used in histopathological researches to assess the degree of hepatic cirrhosis. However, samples taken in liver biopsy only represent 1/50000 of the whole liver. Whether these samples are big and representative enough have been questioned[7]. Furthermore, complications of liver biopsy have made many patients unwilling to accept the procedure, especially for research purposes. These problems can be overcome by taking liver samples from liver resectional specimens. The best and the largest specimen would come from the explanted liver after liver transplantation.
The Ishak grading, which is based on the Knodell’s score, has been considered to be a good method to determine the degree of hepatic fibrosis and cirrhosis on histopathological studies[8]. However, this assessment is still affected by the subjectiveness of the assessors, and it has not been accepted universally as a gold standard[9]. The computer imaging analysis of hepatic fibrosis, which has been developed in the past several years, is able to assess the degree of hepatic fibrosis objectively, quantitatively and accurately[8,10-11].
The objective of this study is to investigate the feasibility of using MELD score to assess the severity of chronic hepatic disease by correlating the pretransplantation MELD score with the degree of hepatic fibrosis in the explanted liver using the computer imaging analysis method, and the degree of cirrhosis by the Ishak grading.
2 Patients and Methods
2.1PatientsThis prospective study was conducted on 58 patients who underwent orthotopic liver transplantation from February to September 2006 at the West China Hospital, Sichuan University. There were 48 men and 10 women. The mean age was 41.8 years (range 24-65). The underlying cirrhosis was due to hepatitis B virus in 56 patients and chronic alcoholism in 2. There were 39 patients with end-stage cirrhosis, 3 with severe chronic hepatitis, and 14 with hepatocellular carcinoma superimposed on cirrhosis. The tumors ranged from 2 to 9 cm in diameter. There were 11 patients with a solitary tumor (4 to 9 cm in diameter), with 8 in the left lobe, 2 in the right lobe and 1 in the caudate lobe; the other 3 patients had multiple tumors (total diameter in each patient was less than 8.5 cm). All the diagnosis accorded with the guidelines set up by the Chinese Medical Association Communicable Diseases and Parasitology Association[12]. The operations performed included the classical orthotopic liver transplantation (n=41), piggyback liver transplantation (n=11), and living donor liver transplantation (n=6, including 5 using a right lobe graft and 1 using a dual graft of the right and the left lobe from two liver donors).
2.2MELDScoreMELD is a numerical model, and the score usually has a decimal value which is rounded to the nearest integer number. The calculation formula is: 3.8 × loge(serum bilirubin, mg/dl) + 11.2 × loge(international normalized ratio of prothrombin time, INR) + 9.6 × loge(serum creatinine, mg/dl) + 6.4 × etiological factor (0 if caused by alcohol or block of bile and 1 if caused by other reasons).
Liver function tests, renal function tests and coagulation profile were performed on the patients on admission to hospital, and the scores were calculated (website http://www. unos.org/ resources). According to the classification by Onaca[13], the scores were grouped into 3 grades: ≤15, 15-25, and>25, respectively.
2.3ComputerImagingAnalysisofHepaticFibrosis
3 × 2 cm2tissue masses were collected from the left lobe of the liver. The samples were immediately fixed in 10% formaldehyde, paraffin embedded, routinely sliced and H&E stained. Masson staining was then used to demonstrate the collagen fibers in blue. For the computer imaging analysis, the total number of blue pixels (indicating collagen fibers) was divided by the total number of pixels of the whole tissue slice to give the area ratio with collagen fibers. In detail, the images of the tissue slices were taken using an Olympus DP70 microscope with a ×10 object lens. For each slice, five images were captured in random at the four corners and the center, respectively. These images were then transferred to the IPP 5.0 image processing system through an OLYMPUS AX70 color camera. In this system, the blue images were converted to two-level yellow ones and the pixel numbers were computed. The average area ratio of liver fibrosis of the 5 images was then calculated to obtain the area ratio of collagen fiber. These steps were performed on all the specimens under the same conditions by the same technician who had no knowledge of the pathological diagnosis of the specimens.
2.4IshakPathologicalGradingThe Ishak pathological grading of chronic hepatitis[14]was used to estimate the degree of cirrhosis. The Ishak modified grading[15]was recorded as follows: 0, no fibrosis; 1, fibrous expansion of some portal tract areas, with or without short fibrous septa; 2, fibrous expansion of most portal tract areas; with or without short fibrous septa; 3, fibrous expansion of portal tract areas with occasional portal-portal bridging; 4, fibrosis with portal-portal and portal-central bridging with occasional nodules; 5, pronounced bridging with visible nodules; and 6, extensive fibrosis and nodules. Not knowing the clinical background of the patients, two experienced hepatopathologists ranked the degree of cirrhosis on the tissue slices, and inter-observer variations between them were evaluated using the Kappa index. When their opinions differed, the opinion of another hepatopathologist was sought.

3 Results
3.1IshakPathologicalGradingandComputerImagingAnalysisThere were 0, 2, 7, 12, 18, 12 and 7 patients in the 7 Ishak grading (0-6), respectively. Inter-observer consistency between the two hepatopathologists was 0.76 for Kappa index, confirming a strong agreement. Computer imaging analysis showed the area ratio of hepatic fibrosis to range from 23.2% to 88.4%, with a mean of 56.7%. There were 9 patients with an area ratio of hepatic fibrosis of 20% to 40%, 32 patients with an area ratio of 41% to 65%, and 17 patients with an area ratio of over 65%.
3.2CorrelationbetweenIshakPathologicalGradingandComputerImagingAnalysisA correlation existed between the Ishak pathological grading and the quantitative computer imaging analysis, (r=0.822,P<0.01), indicating that the area ratio of hepatic fibrosis by the computer imaging analysis increased with the severity of the Ishak grading (Table 1, Figure 1). Furthermore, for the various degrees of hepatic fibrosis the corresponding Ishak grading showed significant difference between the groups (P<0.05) (Table 1).
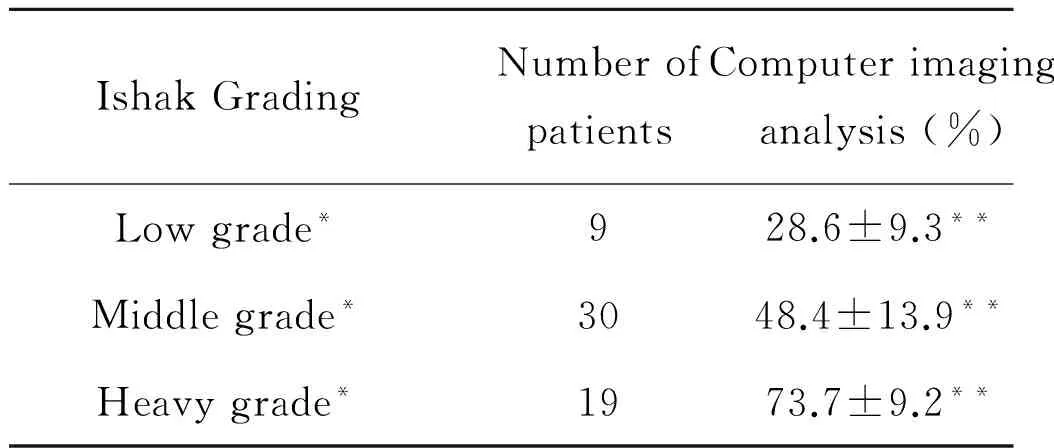
Table 1 Computer Imaging Analysis and Ishak Pathological Grading
*Ishak pathological grading was divided into low, middle and heavy ranks for easy comparison.
**P< 0.05 between any two of the groups.

Fig.1 Scattered chart of correlation between area ratio of hepatic fibrosis and Ishak pathological grading
3.3CorrelationsbetweenMELDScoreandIshakPathologicalGrading/ComputerImagingAnalysisThe MELD score ranged from 11 to 38 (mean±SD, 22.85±9.32). In 10 patients with MELD score between 10 and 15, the mean±SD was 12.4±2.1. In 29 patients with MELD score between 15 and 25, the mean±SD was 20.9±3.6. In 19 patients with MELD score of over 25, the mean±SD was 31.2±6.1. On statistical analysis, the correlation between the Ishak pathological grading and the MELD score was significant (r=0.715,P< 0.01) (Figure 2). The corresponding area ratios of hepatic fibrosis for the various MELD scores were 29.4±8.7%, 46.9±11.6% and 74.3±10.7%, respectively (Table 2). Statistically, there was a significant correlation between the area ratio of hepatic fibrosis and the MELD score, (r=0.838,P<0.01). The higher the MELD score, the larger was the area ratio of hepatic fibrosis and the worse was the cirrhosis. The results indicated that the MELD score accurately reflected the severity of the chronic liver disease (Figure 3).

Table 2 Correlation between MELD Score and Computer Imaging Analysis
*P<0.05 between any two groups.

Fig.2 Scattered chart of correlation between MELD score and Ishak pathological grading

Fig.3 Estimated linear relationship between MELD score and the area ratio of hepatic fibrosis using linear regression
3.4MELDScoreintheAssessmentoftheDegreeofHepaticFibrosisSpearman′s rank correlation test showed that there were good correlations among the area ratio of hepatic fibrosis as determined by computer imaging, the Ishak pathological grading and the MELD score. Linear regression analysis indicated that there was a linear relationship between the MELD score and the area ratio of hepatic fibrosis (Figure 3), with a regression coefficient b=1.868 (95% CI: 1.558 to 2.179). The results indicated that one point increase of MELD score corresponded to 1.87% increase in area ratio of hepatic fibrosis, (statistical analysis of variance,P<0.001). As a consequence the MELD score could be used to evaluate the severity of hepatic fibrosis. Our results also showed the area ratio of hepatic fibrosis was 30% (20% to 40%) for low MELD scores ≤ 15, 50% (35% to 65%) for middle MELD scores between 15 to ≤ 25, and 70% (60% to 90%) for high MELD scores > 25.
4 Discussion
Modern hepatic surgery requires an accurate assessment of the degree of hepatic cirrhosis for prioritization of patients for liver transplantation, for selecting patients for the various treatment strategies, and for prevention and early detection of complications after treatment. Percutaneous needle liver biopsy has been commonly used for the quantitative clinical assessment of hepatic cirrhosis, and it has been considered as a reliable method[9,16-18]. However, it has its inherent limitations. Firstly, liver biopsy is traumatic with its contraindications and complications. Thus, it is not accepted by all patients and it is difficult to repeat again and again. Secondly the sampling process is difficult to standardize. Not long enough or broken specimen often causes error in pathological interpretation and restricts its clinical applications[5,19-21]. Thirdly the uneven distribution of hepatic fibrosis in the liver and the individual variation of the pathologists also limit the accuracy of the assessment of hepatic cirrhosis[8,22]. Other methods, such as radiological techniques and blood biochemical test are helpful, but they have not been validated to be accurate enough to assess the degree of hepatic cirrhosis.
The amount of tissues obtained after liver resection or transplantation is large enough for more thorough pathological studies and some of the limitations of liver biopsy can be overcome. The explanted liver after liver transplantation is an extreme sample that the whole liver can be studied if required. Developed in the past few years, computer imaging analysis can objectively, quantitatively and accurately assess the degree of hepatic fibrosis. Our results showed that the pretransplantation MELD score correlated well with the Ishak pathological grading and with the computer imaging analysis of the degree of hepatic fibrosis in the explanted liver. As the MELD score became greater, the area ratio of hepatic fibrosis became larger, and the Ishak pathological grading became worse. Furthermore, as the area ratio of hepatic fibrosis correlated well with the Ishak pathological grading, the computer imaging analysis could be used to assess the degree of cirrhosis. A strong linear relationship was observed between the MELD score and the degree of hepatic fibrosis (b=1.87,P<0.01) indicating that the MELD score could be used to evaluate the degree of hepatic fibrosis, thus the degree of cirrhosis.
Our results also showed a low MELD score (MELD ≤15) corresponded to 30% (20% to 40%) of area ratio of hepatic fibrosis, a mid MELD score (15
[1] Malinchoc M, Kamath PS, Gordon FD, et al. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts[J]. Hepatology, 2000, 31(4): 864- 871.
[2] Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict poor survival in patients with end-stage liver disease[J]. Hepatology, 2001, 33(2):464-470.
[3] Freeman RB Jr, Wiesner RH, Harper A, et al. The new liver allocation system: moving toward evidence-based transplantation policy[J]. Liver Transpl, 2002, 8(9):851-858.
[4] Brown RS Jr, Kumar KS, Russo MW, et al. Model for end-stage liver disease and Child-Turcotte-Pugh score as predictors of pretransplantation disease severity, posttransplantation outcome, and resource utilization in United Network for Organ Sharing status 2A patients[J]. Liver Transpl, 2002, 8(3):278-284.
[5] Han KH, Yoon KT. New diagnostic method for liver fibrosis and cirrhosis[J]. Intervirology, 2008, 51(Suppl 1) :11-16.
[6] Jaroszewicz J, Rogalska M, Flisiak R. Serum prohepcidin reflects the degree of liver function impairment in liver cirrhosis[J]. Biomarkers, 2008,13(5):478-485.
[7] Addario L, Scaglione G, Tritto G, et al. Prognostic value of quantitative liver function tests in viral cirrhosis: a prospective study[J]. Eur J Gastroenterol Hepatol, 2006, 18(7):713-720.
[8] Beddy P, Lyburn I, Geoghegan T, et al. Outpatient liver biopsy: a prospective evaluation of 500 cases[J]. Gut, 2007, 56(2): 307.
[9] Drebber U, Mueller JJ, Klein E, et al. Liver biopsy in primary biliary cirrhosis: clinicopathological data and stage[J]. Pathol Int, 2009, 59 (8):546-554.
[10] O′Brien MJ, Keating NM, Elderiny S, et al. An assessment of digital image analysis to measure fibrosis in liver biopsy specimens of patients with chronic hepatitis C[J]. Am J Clin Pathol, 2000, 114(5):712-718.
[11] Yin M, Talwalkar JA, Glaser KJ, et al. Assessment of hepatic fibrosis with magnetic resonance elastography[J]. Clin Gastroenterol Hepatol, 2007, 5 (10):1207-1213.
[12] 中華醫(yī)學會傳染病與寄生蟲病學分會, 肝病學分會. 病毒性肝炎防治方案[J]. 中華肝臟病雜志, 2000, 8(6): 324-329.
[13] Onaca NN, Levy MF, Sanchez EQ, et al. A correlation between the pretransplantation MELD score and mortality in the first two years after liver transplantation[J]. Liver Transpl, 2003, 9(2):117-121.
[14] Ishak K, Baptista A, Bianchi L, et al. Histological grading and staging of chronic hepatitis[J]. J Hepatol, 1995, 22(6):696-699.
[15] Zaitoun AM, Al Mardini H, Awad S, et al. Quantitative assessment of fibrosis and steatosis in liver biopsies from patients with chronic hepatitis C[J]. J Clin Pathol, 2001, 54(6):461-465.
[16] Mani H, Kleiner DE. Liver biopsy findings in chronic hepatitis B[J]. Hepatology, 2009, 49 (5 Suppl):S61-71.
[17] Cadranel JF, Castera L, Cales P. Liver biopsy in management of chronic liver diseases: “EASL monothematic conference highlights”[J].Gastroenterol Clin Biol, 2006, 30 (1):121- 123.
[18] Sebagh M, Rifai K, Féray C, et al. All liver recipients benefit from the protocol 10-year liver biopsies[J]. Hepatology, 2003, 37(6):1293- 1301.
[19] Sebastiani G, Halfon P, Castera L,et al. SAFE biopsy: a validated method for large-scale staging of liver fibrosis in chronic hepatitis C[J]. Hepatology, 2009, 49(6):1821-1827.
[20] Soncini M, Leo P, Triossi O, et al. Management and outcomes of hepatic cirrhosis: Findings from the RING study[J]. Hepatology Research, 2006, 36(3):176-181.
[21] Scheuer PJ. Liver biopsy size matters in chronic hepatitis: bigger is better[J]. Hepatology, 2003, 38(6):1356-1358.
[22] Cholongitas E, Quaglia A, Samonakis D, et al. Transjugular liver biopsy: how good is it for accurate histological interpretation?[J]. Gut, 2006, 55(12):1789-1794.
猜你喜歡
甘肅教育(2020年8期)2020-06-11 06:09:46
中華肩肘外科電子雜志(2019年4期)2019-08-24 06:39:12
中華肩肘外科電子雜志(2019年4期)2019-08-24 06:38:46
作文小學中年級(2018年5期)2018-06-11 01:16:12
實用器官移植電子雜志(2018年3期)2018-01-29 15:56:59
公民與法治(2016年10期)2016-05-17 04:13:06
獸醫(yī)導刊(2016年12期)2016-05-17 03:51:27
出版與印刷(2016年3期)2016-02-02 01:20:10
故事作文·高年級(2015年5期)2015-09-08 08:28:19
鄭州大學學報(醫(yī)學版)(2015年1期)2015-02-27 14:50:36
