
Nurses’ engagement in antimicrobial stewardship and its influencing factors: A cross-sectional study
2024-02-27 11:33:40HuiyuNieLiqingYueHunPengJinpingZhouBingyuLiZiweiCo
Huiyu Nie ,Liqing Yue ,Hun Peng ,Jinping Zhou ,* ,Bingyu Li ,Ziwei Co
a Teaching and Research Section of Clinical Nursing,Xiangya Hospital of Central South University,Changsha,Hunan,China
b Xiangya School of Nursing,Central South University,Changsha,Hunan,China
Keywords:
ABSTRACT Objective:This study aimed to investigate the level and influencing factors of nurses’ antimicrobial stewardship (AMS) engagement in China based on the capability,opportunity,motivation,and behavior (COM-B) theory,providing valuable insights for developing effective strategies to improve nursing quality in AMS.Methods:This cross-sectional study was conducted in 17 tertiary hospitals in Hunan,China,from November 2021 to January 2022.A total of 4,514 nurses were selected.The Nurse AMS Engagement Questionnaire (NAEQ),developed using the COM-B theory,was used for evaluation.The questionnaire included capability (14 items),opportunity (7 items),motivation (6 items),and behavior(12 items)four dimensions,39 items.Results:The total NAEQ score was 155.08±27.12,indicating a moderate level.The score of the capability,opportunity,motivation,and behavior dimensions were 52.33 ± 13.48,28.64 ± 5.76,24.57 ± 4.57 and 49.53±8.83,respectively.Significant differences in nurses’AMS engagement were based on professional titles,whether working as a part-time infection control nurse,whether knowing the AMS teams and the defined daily doses of antibiotics,department type,the deployment of clinical pharmacists,and frequency of antimicrobial training and physician-nurse joint rounds (P <0.05).Nurses with junior titles had higher scores on the NAEQ than nurses with intermediate titles (P <0.05).Nurses who worked as part-time infection control nurses,knew the AMS team,and the defined daily doses of antibiotics had higher NAEQ scores than those who didn’t (P <0.01).Nurses working in the ICU and infectious disease department had lower NAEQ scores than those in other departments,such as the ear,nose,and throat (ENT) department (P <0.01).Nurses who had clinical pharmacists deployed in their department had higher NAEQ scores than those without or unclear deployment (P <0.01).Furthermore,nurses who received more frequent antimicrobial training and participated in physician-nurse joint rounds had higher NAEQ scores (P <0.01).Conclusion:Multiple strategies,including enhanced education and training and improved multidisciplinary communication and collaboration,are expected to improve nurse AMS engagement.It is important to give more attention to nurses with intermediate professional titles,less experience,and those working in specific departments.
What is known?
· Nurses’antimicrobial stewardship(AMS)engagement is crucial to successful AMS execution.
· There are few multi-center,theory-based,and comprehensive studies on nurses’ AMS engagement in China.
· The COM-B model has been widely used in research on antibiotic use to understand behavior changes and to guide interventions to optimize antimicrobial prescriptions.
What is new?
· Nurses’ AMS capability in China was at a moderate level,while opportunity,motivation,and behavior were at a relatively high level.
· Nurses’ AMS engagement was mainly associated with professional titles,working as a part-time infection control nurse,knowing the AMS teams and the defined daily doses of antibiotics,department type,the deployment of clinical pharmacists,and frequency of antimicrobial training and physician-nurse joint rounds.
1.Introduction
Antimicrobial resistance (AMR) is among the top 10 global public health crises caused by the overuse and misuse of antimicrobials,which may lead to the resistance of pathogens to antibiotics and ineffective anti-infective treatment [1].Antimicrobial stewardship (AMS),defined as coordinated efforts to promote the appropriate use of antibiotics,represents the cornerstone of the global effort in fighting AMR [2].AMS emphasizes multisectoral participation and multidisciplinary cooperation to achieve the maximum benefits of antibiotic treatment [3].Its significant benefits have been widely demonstrated in several reviews and metaanalyses,which include decreased antibiotic use,delayed drug resistance,reduced antimicrobial-related adverse events,shortened patient hospital stay,and reduced treatment costs [4,5].
China is a large consumer of antibiotics,and AMR was associated with increased mortality,prolonged hospital stays,and additional medical expenses in China [6].To combat AMR,the Chinese government issued multiple policies and plans to promote AMS [7].China’s recent National Action Plan to Contain Antimicrobial Resistance (2022-2025) clearly states that all healthcare staff should receive training on appropriate antimicrobial use,with an accurate knowledge rate reaching over 80% [8].Nurses represent the largest workforce in health care,and their active engagement is crucial to successfully executing AMS [9].Evidence consistently shows that multiple nurse-engaged AMS programs have achieved meaningful outcomes [10,11].Thus,exploring nurses’ engagement in AMS and its associated factors is crucial in providing empirical evidence for developing targeted interventions to improve nursing quality in AMS.
Much research has investigated nurses’ engagement in AMS using various models in multiple countries.A wide range of influencing factors have been identified as barriers or enablers to affect nurses’AMS engagement,which can broadly be classified into two categories: socio-demographic (such as age,gender,education level,title,and working years)and work-related factors(such as the types of hospital and department,previous knowledge,experience,and training of AMS) [12-15].Specifically,AMS-related education and training have been consistently emphasized in almost all studies,with well-established positive effects in improving nurses’AMS engagement and patient outcomes [12-15].However,localized assessment tools based on a theoretical framework are lacking in China to comprehensively examine nurses’ AMS engagement and influencing factors.
In this multi-center,cross-sectional study,we aimed to investigate nurses’engagement in AMS and influencing factors based on the capability,opportunity,motivation -behavior (COM-B) model [16].COM-B is one of the most widely used behavioral science theories to explain the determinants of certain behaviors and guide subsequent behavioral interventions [13,17].COM-B is an overarching model derived from multiple health behavior models such as social cognitive theory,health belief model,and the theory of planned behavior[17].COM-B can explain up to 37%of the variance in behavior,exceeding the predictive validity of other compelling health behavior models[17].COM-B conceptualizes behavior as the result of an interaction between three core elements: capability,opportunity,and motivation [16].For a given behavior to occur,these three factors have to interact over time to shape behaviors in a dynamic system[16].Motivation is a core part of the model,while capability and opportunity influence the relationship between motivation and behavior [16].COM-B has been widely used in research on antibiotic use to understand behavior changes and to guide interventions to optimize antimicrobial prescriptions[18,19].Based on the COM-B model,we aimed to examine nurses’ capability,opportunity,motivation,and behavior of engagement in AMS in tertiary hospitals in Hunan.In addition,we comprehensively compared nurses’ AMS engagement by multilevel factors that included socio-demographic and work-related characteristics.
2.Methods
2.1.Study design and participants
A multi-center,cross-sectional study was conducted among nurses working in tertiary hospitals in Hunan from November 2021 to January 2022.A multistage stratified cluster random sampling was used to determine eligible participants.In the first stage,one prefecture-level city was randomly selected from each of the eastern,western,southern,northern,and central geographic regions of Hunan.In the second stage,at least one general and one specialized tertiary hospital were chosen from each city by purpose sampling.We expanded this method for cities with bigger populations,more hospitals,and more registered nurses,and 17 hospitals were finally selected.
(4)在不同摻砂率混合物中,摻砂率越高其單位質(zhì)量膨潤土中所含NaCl的質(zhì)量越高;又因為摻砂率30%和50%兩種混合物試樣的強度是由膨潤土起主要作用,同時NaCl濃度越高,膨潤土試樣強度越大.因此,在一定濃度的鹽溶液飽和條件下,不同摻砂率混合物試樣的摻砂率越高,其強度及內(nèi)摩擦角越大.
We calculated the sample size according to the formula for the n=z2P (1 -P)/E2,where P represents the cross-sectional study:prevalence of low AMS engagement(the proportion of participants who scored below 80%on the scale).Our pilot investigation showed that the prevalence of low AMS engagement ranged from 38.8%in the motivation dimension to 67.9%in the capability dimension.This study’s sample size calculation was based on the lowest number of 38.8%to allow for maximal power.Z was set as 1.96 at a confidence interval of 95%,and allowable error was fixed as 5%*P,leading to a minimal sample size of 2,424.Considering a rejection or loss-tofollow-up rate of 20%,we expanded our sample size to 3,030.The effective sample size of this study met the requirements.Inclusion criteria of participants included:1)age ≥18,2)licensed nurses with official registration,3)currently employed full-time,4)working in the department with antimicrobial use,and 5)providing direct care to patients with at least one year of work experience.We excluded nurses on leave or working in non-clinical departments.Fig.1 shows the sampling procedure.
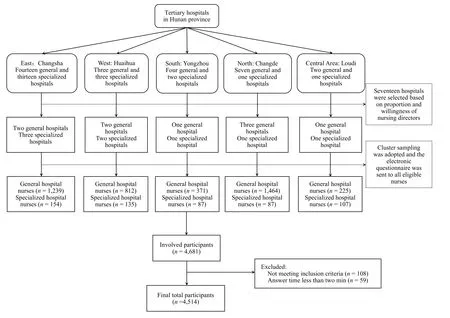
Fig.1. Flowchart of participant selection in tertiary hospitals in Hunan,China.
2.2.Instrument
A self-assessment questionnaire was used to assess participants’general characteristics.It consisted of all potential influencing factors related to nurse AMS engagement under the following two categories based on the literature review [12-15]: 1) sociodemographic factors,including gender,age,professional title,years working as a nurse,and education degree;2) work-related factors,including whether working as a part-time infection control nurse,whether knowing the AMS team,whether knowing the defined daily doses of antibiotics,hospital type,department,deployment of clinical pharmacists in the department,frequency of antimicrobial training,and frequency of physician-nurse joint rounds.
The study utilized the Nurse AMS Engagement Questionnaire(NAEQ),which was designed based on the COM-B theory [16,20].This questionnaire was developed via a literature review,semistructured interviews,and two rounds of expert consultation.Details of the questionnaire development and initial validation have been described elsewhere in Chinese [20].The questionnaire consisted of 39 items and 4 dimensions: capability (14 items),opportunity(7 items),motivation(6 items),and behavior(12 items).Each item is rated on a 5-point Likert scale from 1 strongly disagree/ never) to 5 (strongly agree/always).Each dimension’s total score ranges from 14-70,7-35,6-30,and 12-60,respectively,with a higher score indicating a higher level of AMS capability,opportunity,motivation,and behavior.For easy comparison with other studies using different measurement tools,we transformed the questionnaire scores into percentages using the modified Bloom’s categorization for scores[21,22].According to this study,nurses had a“high”level of AMS engagement if the score ranged between 80%and 100% (156-195 points for NAEQ,56-70 points for capability dimension,28-35 points for opportunity dimension,24-30 points for motivation dimension,and 48-60 points for behavior dimen-sion);“moderate” if the score was between 50% and 79% (98-155 points for NAEQ,35-55 points for capability dimension,18-27 points for opportunity dimension,15-23 points for motivation dimension,and 30-47 points for behavior dimension);and“l(fā)ow”if the score was less than 50%(39-97 points for NAEQ,14-34 points for capability dimension,7-17 points for opportunity dimension,6-14 points for motivation dimension,and 12-29 points for behavior dimension).Good reliability was established by the content validity index of 0.97 and the Cronbach’s α coefficient of 0.96 for the total scale and 0.92-0.94 for its four dimensions [20].
2.3.Data collection
The survey was posted on Wenjuanxing(https://www.wjx.cn/),China’s biggest online questionnaire design,distribution,and data collection platform.Research assistants who underwent unified and standard research training were assigned to each hospital.They first contacted the nursing directors,explained the study objectives,and assisted in advertising the survey.After obtaining approval from the nursing directors,a survey link or QR code containing the questionnaire was sent to the head nurses,who then forwarded it to the department nurse WeChat group.It took an average of 15 min to complete the questionnaire,and each IP address was limited to one response to avoid repeated submission.
2.4.Data analysis
Data were analyzed using IBM SPSS version 26.Continuous variables were described using means and standard deviations,whereas categorical variables were presented using frequencies and percentages.All data were normally distributed.We used twosample independent t-tests for two-group comparisons,with a Pvalue <0.05 considered statistically significant.We used one-way ANOVA for multiple-group comparisons,followed by Post Hoc Tests using the LSD Method,with adjusted P-values by Bonferroni corrections.
2.5.Ethical considerations
This study was approved by the Behavior Medicine and Nursing Ethics Review Committee of Xiangya School of Nursing of Central South University (ID: E202161).All eligible nurses participated in the survey voluntarily and provided electronic informed consent before completing the questionnaire.All participants were informed that no private information was collected,and the study procedure followed rigorous rules to ensure confidentiality,privacy,and anonymity.
3.Results
3.1.Participants characteristics
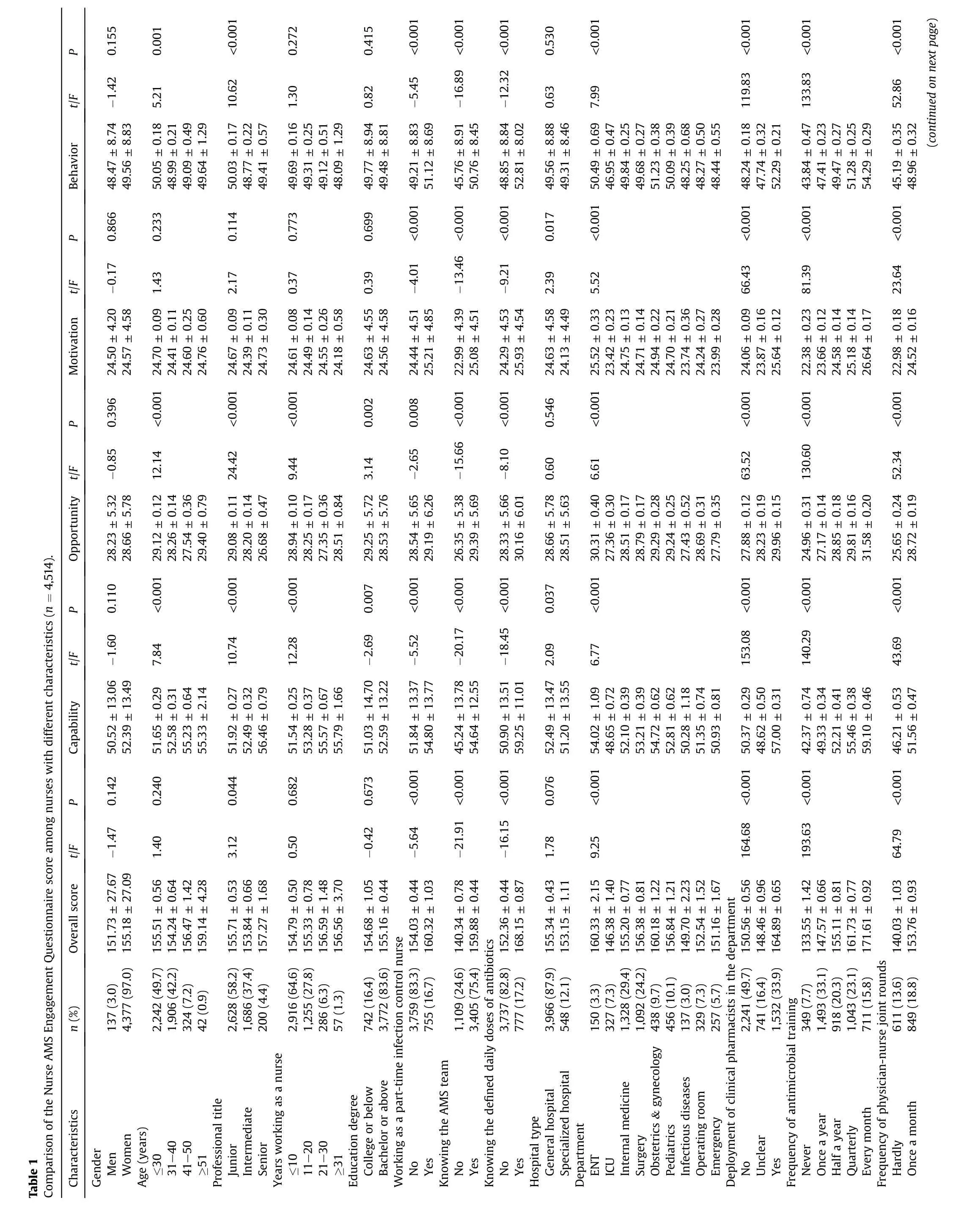
Most of the respondents were female (n=4,377,97.0%) who worked under a junior professional title(n=2,628,58.2%)and held a bachelor’s degree or above(n=3,772,83.6%).Their mean age was 31.42 years,with an average of 9.93 years of work experience.A total of 755(16.7%)respondents also worked as part-time infection control nurses.Although the majority of nurses (n=3,405,75.4%)knew the AMS teams,only a minority of them(n=777,17.2%)were aware of the defined daily doses of antibiotics.Most participants were from general hospitals(n=3,966,87.9%).Regarding the work department,about half of the participants were from medicine and surgery (n=2,420,53.6%).Only one-third of nurses (n=1,532,33.9%) acknowledged the deployment of clinical pharmacists in their department.A total of 349 (7.7%) nurses had never received AMS training,and 611 (13.6%) worked in a department without joint ward rounds(Table 1).
3.2.Overall status of the nurse AMS Engagement Questionnaire
The overall NAEQ score was 155.08±27.12,indicating a moderate level.The score of the four dimensions of capability,opportunity,motivation,and behavior were 52.33 ± 13.48,28.64 ± 5.76,24.57±4.57,and 49.53±8.83,respectively,which represent a moderate level of AMS capability and a relatively high level of AMS opportunity,motivation,and behavior.Capability dimension included 14 items,among which the highest-scored item was related to the management of adverse reactions to commonly used antimicrobials (C12),while the three lowest-scored items were associated with the knowledge of infection assessment,diagnosis,treatment,and awareness of AMS policy (C4,C3,C2).Opportunity dimension consistedof7items,amongwhichthehighest-scoreditemwas“hospitals encourage nurses to report antimicrobial-related adverse events or adverse reactions” (O4),while the two lowest-scored items were “hospital policy advocacy of nurse engagement in AMS” (O1) and “opportunities of participating in multidisciplinary clinical activities”(O2).Motivation dimension included 6 items,among which the lowest-scored item was related to advocating patient engagement in AMS (M3),while the highest-scored item was associated with responsibilities of collaborative AMS (M1).Behavior dimension included 12 items,among which the two lowest-scored items were linked to participation in multidisciplinary consultations of infection cases (B2) and antimicrobial discussions (B12),while the highestscored item was regarding collecting specimens of pathogenic microorganisms correctly(B6)(Table 2).
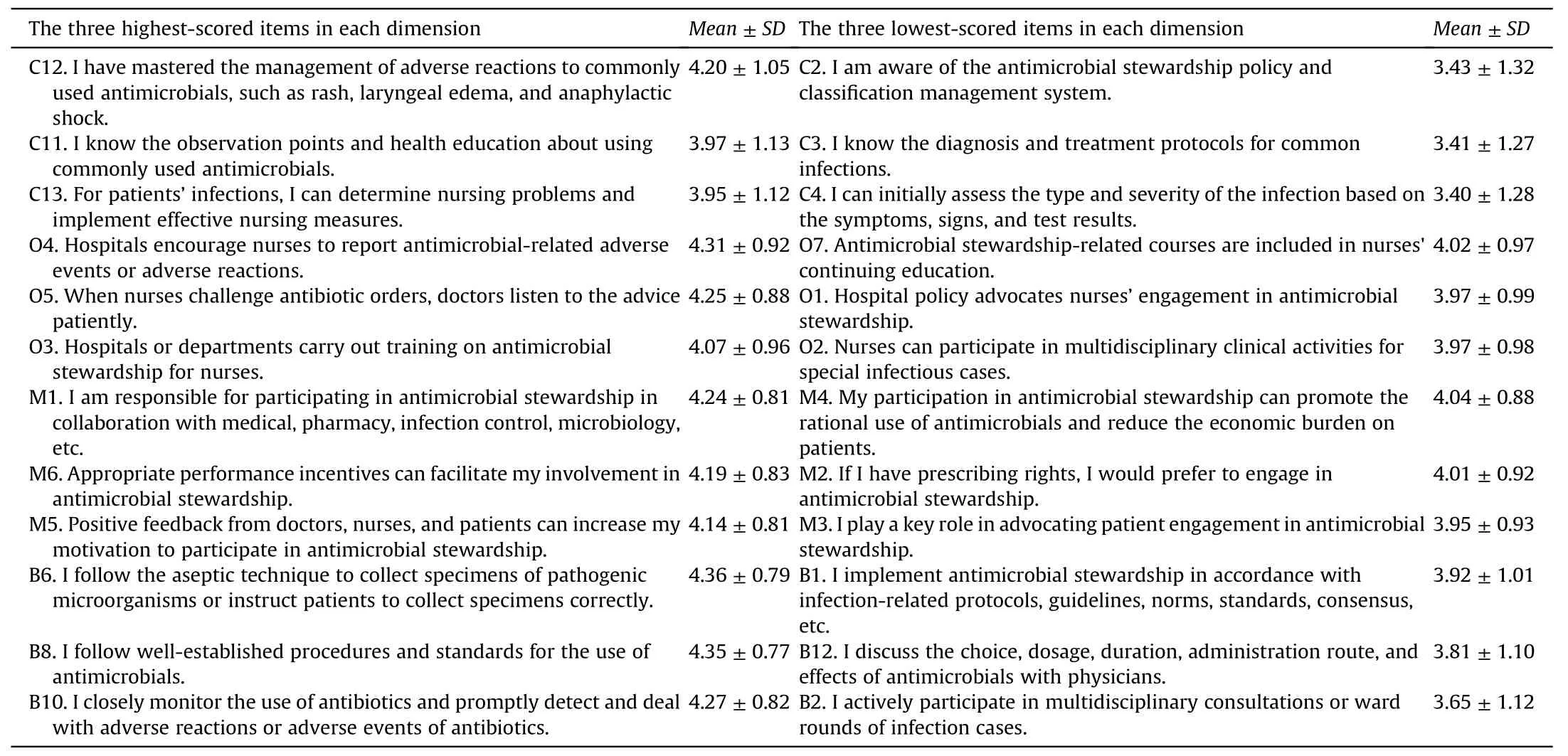
Table 2 The three highest and lowest-scored items in capability,opportunity,motivation,and behavior dimensions (n=4,514).
3.3.Influencing factors of AMS engagement among nurses
There were significant differences in the total NAEQ by the following eight factors: professional titles,whether working as a part-time infection control nurse,whether knowing the AMS team,whether knowing the defined daily doses of antibiotics,department type,deployment of clinical pharmacists in the department,frequency of antimicrobial training,and frequency of physiciannurse joint rounds (P <0.05).The pairwise comparison results were as follow.Nurses with junior titles had higher NAEQ scores than nurses with intermediate titles(P <0.05).Nurses who worked as part-time infection control nurses,knew the AMS team,and knew the defined daily doses of antibiotics had higher NAEQ scores than those who didn’t (P <0.01).Nurses in the ICU and infectious disease department had lower NAEQ scores than those in other departments,such as the ear,nose,and throat (ENT) department (P <0.01).Nurses with deployment of clinical pharmacists in the department had higher NAEQ scores than those without or unclear deployment (P <0.01).In addition,nurses with more frequent antimicrobial training and physician-nurse joint rounds had higher NAEQ scores(P <0.01).(Table 1).
For each dimension of the NAEQ,capability dimension scores showed statistically differences by all socio-demographic and work-related factors except for gender.Besides,opportunity dimension scores showed statistically differences in all sociodemographic and work-related characteristics except gender and hospital type.Motivation dimension scores showed statistically differences by all work-related factors but not socio-demographic factors.In addition,behavior dimension scores showed differences by age,professional title,and all work-related factors except hospital type (Table 1).
4.Discussion
This study found that nurses had moderate levels of AMS engagement,suggesting that there is much room for improvement in the quality of care related to AMS.Our study showed that the three lowest-scored items of nurse AMS capability were related to the knowledge of infection assessment,diagnosis,treatment,and awareness of AMS policy.Our results identified a lack of knowledge as the main obstacle to nurse engagement in AMS,consistent with the findings from other countries that consistently show low levels of AMS knowledge [23-25].These findings emphasize the lack of AMS knowledge worldwide and indicate the urgent need to strengthen AMS nursing education and training.Our conclusion that nurses had low awareness of AMS protocols and policies was similar to Kirby et al.’s study,which showed that nurses felt excluded from education about new prescribing policies[26].Thus,nurses should be involved in developing,implementing,and training AMS guidelines and policies to empower their antimicrobial decisions and enhance their AMS capabilities.
For the opportunity dimension,the two lowest-scored items were related to the lack of policy to engage in AMS and the opportunity to participate in multidisciplinary activities;previous studies showed that both were critical enablers of AMS nursing quality [11,27].Nurses play an essential role in AMS involvement and multidisciplinary collaboration,and strong administrative support and more opportunities are required to improve their engagement.A national survey in China showed that the AMS leadership committee paid little attention to nursing staff [28].Therefore,stewardship leaders should acknowledge nurses’ value in AMS policies and explore supporting measures such as inviting nurses to participate in the AMS committee and integrating AMS teamwork into nursing routines [29].
In general,nurses showed high motivation(24.57±4.57)in AMS engagement in our study,comparable to that reported in other countries [21,30].The highest-scored item was related to nurses’sense of responsibility,indicating responsibility may be a primary driver of nurses’AMS engagement and that it is necessary to define nurses’ responsibilities in AMS policies.Nurses expressed the lowest motivation in engaging patients in AMS,indicating much room for improvement in encouraging nurses to strengthen their communication with patients and families and provide patient education on AMS.
For the behavior dimension,the two lowest-scored items were related to multidisciplinary consultation and discussion with physicians.In general,nurses had high compliance with the current protocols and guidelines in AMS,which may reflect the successful implementation of the National Action Plan on AMS in China.As shown in our study,nurses performed well in independent AMS practices,such as microbial specimen collection,best practices of antimicrobial use,and patient education.Previous studies showed that these roles had been well perceived and recognized [31].However,our results revealed nurses’ poor engagement in multidisciplinary AMS activities and discussions with physicians on appropriate antimicrobial prescriptions.This may be due to the deeply rooted professional boundaries between nurses and physicians/pharmacists,including prescribing capability,power/authority,and responsibility that prevent nurses’ participation in multidisciplinary collaborations [32].Other reasons may include a lack of role perception,knowledge,and time.These findings suggest that more policies and support are needed to encourage nurses’ communication and collaboration with other health professionals to improve their multidisciplinary AMS engagement.
Our study revealed that nurses with junior professional titles had higher AMS engagement,which may be related to junior nurses’young age and more openness and enthusiasm to learn and practice AMS.This suggests nurses with higher professional titles should be motivated and encouraged to learn and engage AMS.In addition,nurses who had previously worked as part-time infection control nurses also had higher AMS engagement than those with no work experience.This finding suggests that involving nurses in different departments in infection control work may be an excellent way to improve their AMS engagement.Furthermore,our study showed that nurses who knew the AMS team and the defined daily doses of antibiotics had significantly higher scores of AMS engagement.This result was consistent with previous findings showing a positive relationship between familiarity with AMS and engagement in AMS [25].These findings suggest that hospitals should establish and advertise AMS teams and strengthen nurses’education and training on antimicrobial prescriptions to improve their engagement in AMS.
Nurses working in the ICU and infectious disease department had lower AMS engagement than nurses in other departments,such as the ENT department.The relatively heavier workloads may explain this,as well as a more severe shortage of nursing staff and more obvious professional boundaries in the ICU and infectious disease department,which are well-established barriers to nurses’ AMS engagement[33].These findings suggest that more attention should be paid to nurses in specific departments,with training,staffing,and collaboration provided when needed.Additionally,our study revealed that deploying clinical pharmacists in the department was associated with higher nurse AMS engagement.This result was similar to a previous study in Korea,showing that nurses with easy access to infectious disease specialists had more insightful attitudes about antimicrobial use and resistance and,thus,better AMS engagement[34].Considering the shortage of clinical pharmacists in China,it is imperative to improve the education system of clinical pharmacy and share clinical pharmacists with multiple wards,which may help enhance nurses’engagement in AMS.
Our study showed that nurses with frequent AMS training had higher AMS engagement.This result was consistent with previous studies demonstrating that training improved nurses’ and nursing students’ knowledge,attitudes,and beliefs of AMS [35].It can be explained by utilizing the “COM-B” model,i.e.,capability and opportunity impact motivation;capability,opportunity,and motivation impact behavior [16].These findings further highlight the importance of providing intensive and continuous AMS training for nurses to improve their AMS engagement.In addition,our study demonstrated that more frequent physician-nurse joint rounds were associated with higher AMS engagement.This finding aligned with previous interventional studies showing that incorporating nurses into AMS and infection prevention rounds decreased antimicrobial use [10,27].Joint rounds enable bidirectional communication and mutual learning between nurses and physicians about preventing,diagnosing,and treating infections.Besides,the joint round was cost-effective and accessible.This finding suggests that ward managers should consider including physician-nurse joint rounds into work routines to improve nurses’engagement in AMS.
This study has several limitations.First,all data collection was based on the self-report survey,which is subject to social desirability bias and may result in nurses reporting higher levels of AMS capability,opportunity,motivation,and behavior.Second,our study samples were recruited from tertiary hospitals in Hunan and may not represent other hospitals.Third,the online survey method may have excluded nurses who encountered difficulties using the internet or answering an online survey.Of note,the study was performed during the pandemic,which may be a limitation due to unusual work conditions for most nurses.
5.Conclusion
This study reveals that nurse AMS engagement was at a moderate level.Our findings provide important implications for future research and intervention programs to improve nurses’ AMS engagement through multiple strategies,such as strengthening education and training and improving multidisciplinary communication and collaboration.Besides,more attention should be paid to nurses with intermediate professional titles,less experience,and working in specific departments in designing intervention programs to improve nurses’ AMS engagement.
CRediT authorship contribution statement
Huiyu Nie:Conceptualization,Methodology,Data Curation,Formal analysis,Investigation,Writing-original draft,Writingreview &editing.Liqing Yue:Conceptualization,Methodology,Data Curation,Investigation,Resources,Supervision,Writingreview &editing.Huan Peng:Methodology,Data Curation,Project administration,Writing-original draft,Writing-review &editing.Jinping Zhou:Conceptualization,Methodology,Data Curation,Project administration,Writing-original draft,Writing-review &editing.Bingyu Li:Data Curation,formal Analysis,Investigation,Writing-original draft,Writing-review &editing.Ziwei Cao:Data Curation,formal Analysis,Investigation,Writing-original draft,Writing-review &editing.
Funding
Nothing to declare.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of competing interest
The authors declare that they have no competing interests.
Acknowledgements
We would like to express our gratitude to all collaborating participants.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.12.002.
猜你喜歡
西部交通科技(2023年10期)2024-01-08 07:19:50
建材發(fā)展導向(2022年12期)2022-08-19 02:31:24
江蘇建材(2021年2期)2021-05-12 01:19:58
礦產(chǎn)綜合利用(2020年1期)2020-07-24 08:51:42
電鍍與環(huán)保(2017年6期)2018-01-30 08:33:30
數(shù)理化解題研究(2017年4期)2017-05-04 04:08:05
硅酸鹽通報(2016年10期)2016-12-22 06:46:16
水利規(guī)劃與設(shè)計(2016年7期)2016-02-28 15:06:39
應(yīng)用化工(2014年1期)2014-08-16 13:34:08
建筑材料學報(2014年1期)2014-03-11 17:07:21
 International Journal of Nursing Sciences2024年1期
International Journal of Nursing Sciences2024年1期
- International Journal of Nursing Sciences的其它文章
- Editorial Board of International Journal of Nursing Sciences
- Chinese Abstract
- Corrigendum to “Relationship between nurses’ perception of professional shared governance and their career motivation in Egypt:A cross-sectional study” [Int J Nurs Sci 10/4 (2023) 485-491]
- 《國際護理科學(英文)》進入中科院分區(qū)護理類2 區(qū)
- 關(guān)于翻譯量表使用授權(quán)的問答
- Summary of Guide for Authors