
Autoimmune complications and clinical outcomes of herpes simplex encephalitis in children: A case series
2023-06-26 09:37:02DemetKayaoraElifrkanUygurahinEnesSalGoncaBekta
Gül Demet Kaya ?z?ora, Elif S?bü, Türkan Uygur ?ahin, Enes Sal?, Gonca Bekta?
1Department of Pediatric Neurology, Health Sciences Faculty, Hasan Kalyoncu University, Gaziantep, Turkey
2Department of Pediatric Endocrinology, Kartal Dr.Lutfi Kirdar City Hospital, Istanbul, Turkey
3Department of Pediatric Neurology, Bezmialem University Medical Faculty, Istanbul, Turkey
4Department of Pediatric Infectious Diseases, Umraniye Research and Training Hospital, Istanbul, Turkey
5Department of Pediatric Neurology, Boston Children's Hospital, Boston, USA
ABSTRACT Objective: To report the neurologic prognosis and autoimmune complications of 16 cases of childhood herpes simplex virus encephalitis.Methods: The study was conducted at ?anl?urfa Training and Research Hospital, Turkey from June 2017 to August 2019.The study included 16 pediatric patients aged between 6 months and 17 years (median age 77.7 months) who were diagnosed with herpes simplex virus type 1 encephalitis by pediatric infectious disease and pediatric neurology clinics.Patients were followed using patient records, and interviews at the pediatric neurology clinic or via the telephone.Clinical and demographic data, received therapies,neurologic prognosis and complications were evaluated.Results: Patients with and without autoimmune encephalitis were compared in terms of age, sex, symptom duration before treatment,initial cerebrospinal fluid protein, glucose, red blood count and white blood count but no significant difference was found.Autoimmune complications were seen in four patients.N-methyl-D-aspartate encephalitis was observed in three patients and choreoathetosis was seen in one patient.The average follow-up period was 48.3 months.Twenty-five percent of the patients were receiving multiple antiepileptic drug (AED) treatment, 43.8% were receiving single AED treatment and 31.3% were not receiving AED treatment at the end of the follow-up.Motor disability was observed in 12.5% and drug-resistant epilepsy was observed in 6.3% who had autoimmune complications.Conclusions: Seizures and movement disorders were controlled with immunotherapy and autoantibodies should be studied routinely.Treatment should be started early upon recognition of autoimmune complications through follow-up by measuring autoantibody levels and clinical examination results.Effective prevention and curative treatment modalities are needed to avoid herpes simplex virus encephalitis complications.
KEYWORDS: Herpes simplex virus encephalitis; Autoimmune complications; Epilepsy; Children; Steroid; Prognosis
1.Introduction
Encephalitis is an inflammation of the brain parenchyma associated with clinically diagnosed neurologic dysfunctions that can be caused by viral, post-infectious or non-infectious etiologies.Herpes simplex virus encephalitis (HSE) is the most common cause of sporadic fatal encephalitis with a worldwide incidence of 2-4 cases per million people per year[1-3].It is a morbid disease with a 70% mortality rate in the absence of treatment, a mortality rate of 10%-30% despite treatment and a recurrence rate of 10%.Most HSEs are caused by herpes simplex virus (HSV) type 1 (90%)and rarely by HSV-2 (10%).HSV-2 mostly occurs in neonates and immunosuppressed patients[1-3].Viruses enter the body through the oropharyngeal mucosa, conjunctiva and damaged skin.Although it seems reasonable to assume that host factors such as age and immunodeficiency as well as interactions between host and virus are the main determinants of the disease’s phenotype, neurovirulence of herpesviruses should also be considered.More than two-thirds of herpes simplex virus type 1 (HSV-1)-related infections are caused by the reactivation of endogenous latent HSV-1 in individuals previously exposed to the virus, whereas the remaining infections result from primary infection in individuals who were not previously exposed to HSV.Some studies suggest that HSE is more commonly caused by primary infection than reactivation[1-5].
HSV polymerase chain reaction (PCR) tests in cerebrospinal fluid (CSF) are the gold standard in diagnosis with a sensitivity of 98% and specificity of 94%.Electroencephalography (EEG)and magnetic resonance imaging (MRI) are also highly diagnostic regardless of CSF findings.A cranial MRI typically shows unilateral medial temporal, insular, cingulate lobe and frontobasal cortex involvement while an EEG shows periodic lateralized discharges and slowing ground activity.Post-HSE complications are motor disability, learning and memory problems, behavioral disorders,sleep disorders, recurrent headaches and epilepsy.Autoimmune complications have also been observed in recent years[1-5].Autoimmune encephalitis is an autoimmune complication that increasingly recognized neuropsychiatric condition seen in patients of all ages.Herpesvirus infections of the brain can precede the development of pathogenic autoantibodies against N-methyl-Daspartate receptors (NMDAR) and further neuronal surface proteins which leads to neuronal dysfunction and relapsing symptoms[6,7].Our future expectations for HSE should not be restricted to reducing mortality but also to reducing short and long-term sequelae.Our study aimed to report the neurologic prognosis and autoimmune complications of 16 cases of childhood HSE which will assist further studies on this subject.
2.Subjects and methods
This was a single centre retrospective study at the ?anl?urfa Training and Research Hospital, in Turkey.This study had received approval from the Health Research Ethics Committee of Harran Universty with number HRU.19.05.23.Informed consent was obtained.
The inclusion criteria of this study were children who were diagnosed as having HSV-1 encephalitis by pediatric infectious disease and pediatric neurology clinics from June 2017 to August 2019 and HSV-1 encephalitis patients aged under 18 years old.The diagnosis of HSE was made in the presence of CSF PCR test positivity,clinical and radiologic findings.Patients were followed until 2022 using patient records, interviews at the pediatric neurology clinic and telephone interviews.The median follow-up period was 48.3 months.Clinical and demographic data, received therapies, neurologic prognosis and complications were evaluated.Initial MRI examinations were performed and the initial EEGs of all patients were examined within two days of admission.MRI scans were performed at two main sites using a 1.5 Tesla Siemens Aera scanner.The protocol consisted of the following scan sequences: sagittal T1-weighted spin-echo, slice thickness=1.0 mm, axial T2-weighted fast spin-echo, coronal oblique fast fluid-attenuated inversion recovery and axial diffusion-weighted single shot spin-echo-planar.EEGs were performed during the sleepwake cycle using 21 electrodes; including Fp1, Fp2, F3, F4, F7, F8, T3,T4, T5, T6, C3, C4, P3, P4, O1, O2, Fz, Cz, Pz, a ground electrode and a reference electrode.An initial EEG was performed within the first 48 hours in all patients.The electrodes were placed according to the international 10-20 system and a Nihon Kohden EEG device was used for recording.All patients were given intravenous acyclovir at 15 mg/kg for every eight hours concomitantly for 21 days.Follow-up CSF HSV PCR tests were performed in all patients.Antiepileptic drug (AED)treatment was started with presence of seizure or EEG abnormality accompained by consciousness.Multiple AEDs were started in patients with recurren seizures.AMPA1, AMPA 2, ANTI-CASPR2, ANTI-LGI 1, ANTI-GABA B (GABABARB1/B2), ANTI-DPPX and NMDA antibodies were studied using the indirect immunofluorescent antibody method in CSF of cases of suspected autoimmune encephalitis.Antiepileptic treatment reduced after the four-fifth year in patients with normal EEGs and without recurrence of seizures.
The data were evaluated in the package program of IBM SPSS Statistics Standard Concurrent User V 26 (IBM Corp., Armonk, New York, USA).Descriptive statistics were given as number of units(n), percent (%), median and interquartile range (IQR).The normal distribution of the data of numerical variables was evaluated with the Shapiro Wilk test of normality.Comparisons between groups for numerical variables were made with the Mann-Whitney U test.Comparisons between groups for the sex variables were made with Fisher’s exact test.A P value of <0.05 was considered statistically significant.
3.Results
The study included 16 pediatric patients with 11 boys and 5 girls,aged between 6 months and 17 years (median age: 77.7 months).The average follow-up period was 48.3 months.All patients were found to be positive for HSV-1 in CSF PCR tests.The mean time between the onset of symptoms and the start of therapy was 3.1 days.Symptoms duration before treatment in patients with autoimmune complications was 4 days and without autoimmune complications was 3 days.No significant difference was found between them(P=0.379).Presenting symptoms included fever, seizures, altered state of consciousness, nausea and amnesia (Table 1).Fifteen of the patients (93.8%) had seizures and all had a fever.Confusion was seen in 75% of patients with autoimmune complications.
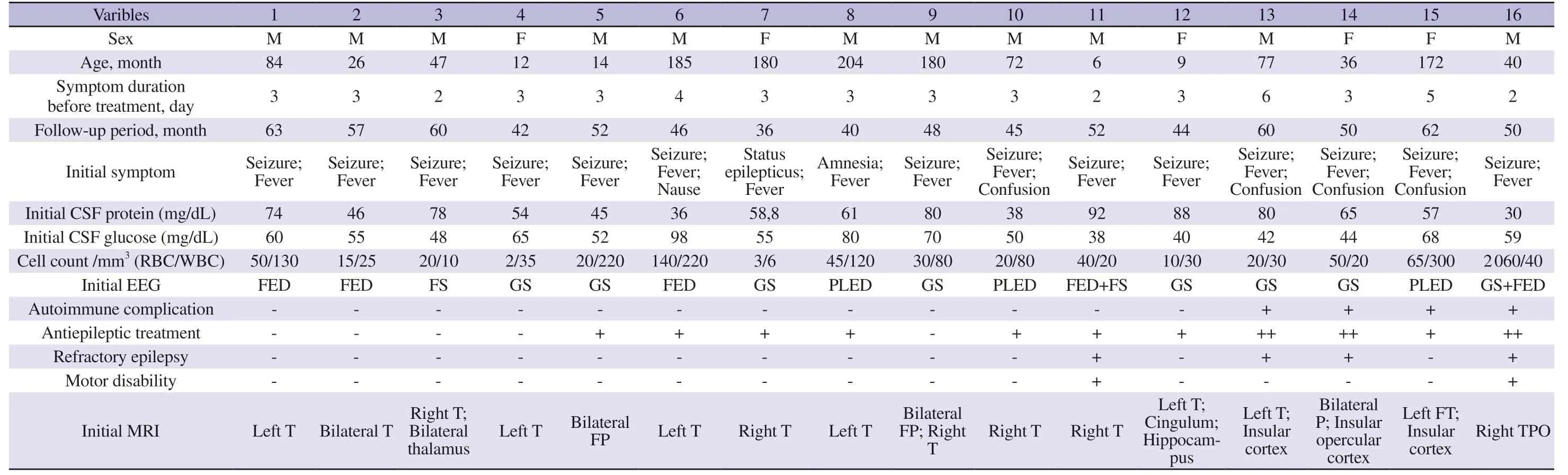
Table 1.Demographic, clinic and laboratory findings.
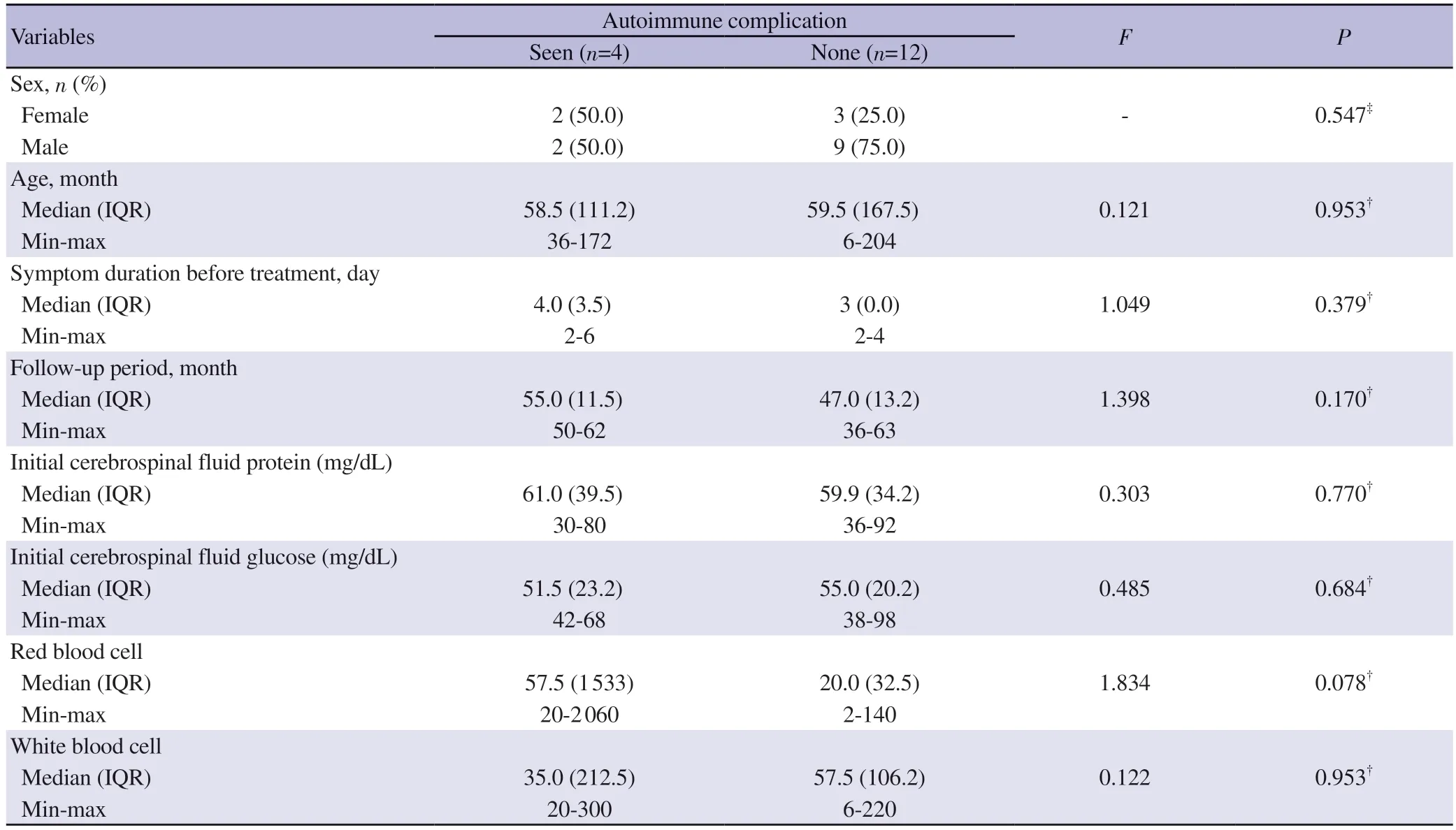
Table 2.General characteristics of the groups.
Lumbar puncture was performed in all patients at the time of diagnosis and on day 20 and day 21.The mean initial CSF findings in patients with autoimmune complications were CSF protein 61 mg/dL; glucose 51.5 mg/dL; red blood cells (RBC) 57.5 cells/mm3;white blood cells (WBC) 35 cells/mm3; in those without autoimmune complications, these findings were CSF protein 59.9 mg/dL; glucose 55 mg/dL; RBC 20 cells/mm3; WBC 57.5 cells/mm3.There was no significant difference in CSF protein (P=0.770), glucose (P=0.684),RBC (P=0.078) and WBC (P=0.953) between patients with and without autoimmune complications.There were no statistically significant differences in terms of age and sex between patients with and without autoimmune complications.
All patients were given intravenous acyclovir at 15 mg/kg every eight hours concomitantly for 21 days.All patients were given a meningitis dose of broad-spectrum antibiotics until the CSF PCR and culture test results were available (ceftriaxone, vancomycin or meropenem).Clinical worsening or resistance to treatment was not observed in any patients under acyclovir treatment.
Multiple AEDs were given in four patients (patients 12, 13, 14, 16)due to seizure recurrence in the acute period and status epilepticus was not observed.Levetiracetam and phenytoin were the first preferred antiepileptics due to their availability and safety.Patient 8 did not have clinical seizure but was treated with levetiracetam because of memory loss and periodic lateralized epileptic discharges on EEG.
In the initial EEGs, periodic lateralized discharges were observed in three patients (18.8%), focal epileptiform discharges were observed in five patients (31.3%) and generalized or focal slowing at delta frequency was observed in ten patients (62.5%).
Isolated unilateral temporal involvement was observed in seven patients (43.8%), and bilateral temporal involvement was observed in one patient (6.3%).Eight patients (50%) had diffuse (frontal lobe,parietal lobe, thalamus, hippocampus, cingulate gyrus, or insula)involvement in addition to temporal involvement.On follow-upMRIs sequelae changes in the form of gliosis and encephalomalacia were detected in all patients.
The average follow-up period was 48.4 months.The mean followup period of five patients (31.3%) were 54 months at which point their EEGs were normal and there was no recurrence of seizures.They were not receiving antiepileptic treatment as one patient(patient 4) discontinued therapy voluntarily.Seven patients (43.8%)had a mean follow-up time of 47.5 months and were receiving monotherapy.Antiepileptic treatment was continued in these groups due to the presence of epileptic activity in EEG or seizure recurrence.Five patients (31.3%) were receiving multiple AEDs and had a mean follow-up period of 51 months.The EEGs of these patients were abnormal and the seizures could not be controlled with monotherapy.Two patients (12.5%, patient 14 and 16) had the motor disability as spastic tetraplegia.Autoimmune complications were seen in four patients (25.0%).Anti-N-methyl-D-aspartate receptor encephalitis (NMDARE) was observed in three patients (18.8%) and choreoathetosis was observed in one (6.3%).Patients with NMDARE presented to complaint with choreiform movement disorder after six weeks of HSE (patient 13), orofacial dyskinesia and dystonia after three weeks (patient 14) and self-mutilation and psychosis after five weeks (patient 15).Choreoathetosis was observed on day 20 in patient 16.All patients underwent lumbar puncture as well as HSV PCR tests and autoimmune encephalitis panel analyses.All patients tested negative for follow-up HSV PCR.MRIs were performed and new involvement was not observed.
Patient 13 received pulse steroid therapy for 3 days (gradually tapered and stopped in 4-6 weeks) which was followed by intravascular immunoglobulin (IVIG) therapy for six months.IVIG treatment started due to refractory seizures in patient 13.Patient 15 received pulse steroid treatment which tapered gradually for six weeks.Patient 14 received pulse steroid, plasmapheresis, IVIG and rituximab therapy.Second-line treatment was started after 4 weeks due to refractory seizures.Patient 16 received only IVIG therapy.
Patient 13 had mild cognitive impairment and epilepsy, patient 14 had severe cognitive impairment and refractory epilepsy, patient 15 had mild cognitive impairment and patient 16 had motor disability with severe cognitive impairment and epilepsy.
At the chronic stage, MRIs revealed left temporal and insular encephalomalacia in patient 13, bilateral frontotemporal and insular volume loss in patient 14, left temporo-occipital and incular encephalomacia in patient 15 and right temporo-parieto-occipital and incular encephalamalacia in patient 16.Diffuse involvement in MRI was observed in eight patients (50.0%).There was diffuse involvement in all patients with autoimmune complications and there was diffuse involvement in four (25.0%) patients without autoimmune complications.Autoimmune complications were observed in three of four (75.0%) patients who were admitted with the symptom of confusion.
4.Discussion
Encephalitis is a serious public health problem due to its high morbidity and mortality.Viruses are the most common cause of encephalitis.HSE is the most common cause of sporadic encephalitis[8].Despite acyclovir treatment, the rate of continuing daily life activities after HSE is only 40%-55%.It is uncertain if all poor outcomes are due to viral cytopathology or whether it is accompanied by immune-mediated pathogenesis[9-13].Early recognition and treatment are very important to decrease mortality.Fever, headache, seizure, focal neurologic deficit and altered of consciousness are the main clinical presentations of HSE.Headache and altered consciousness in the adult age group are the most common presentations.Consistent with studies in the pediatric age group, seizure and fever were the most common symptoms in our study.We believe that presentation with seizures is more common due to neuronal hyperexcitability in the immature brain[14].
A long interval between treatment and symptom onset, the presence of signs of meningeal irritation, severely depressed levels of consciousness, an age younger than four years and widespread involvement in MRIs have been reported as factors associated with poor prognosis[15].One of the factors affecting the prognosis in HSE is the early initiation of effective antiviral therapy.In the presence of clinical suspicion, it is recommended to start empirical treatment as early as possible.In adult studies the duration of starting therapy is 6.1 days[16].
In earlier reports, nephrotoxicity was the most common adverse effect (12%-48%) of acyclovir treatment[17].In our study,nephrotoxicity was observed in a patient after a contrast-enhanced brain MRI before acyclovir treatment (patient 7).A diagnosis of acute nephrotoxicity, hypertension and related posterior reversible encephalopathy syndrome was seen.Renal function was reversible with adjustment of the acyclovir dose and increased hydration with antihypertensive therapy, while acyclovir-induced nephrotoxicity was not observed.
N-methyl-D-aspartate encephalitis is the most common cause of non-viral encephalitis that can be triggered by HSV.There are several studies indicating that HSE can trigger an immune-mediated inflammatory phase with associated NMDAR antibodies.NMDARE is an autoimmune type of encephalitis that can show acute or subacute course and is characterised by psychiatric symptoms such as seizures, psychosis, catatonia, agitation, dyskinesia, movement disorders (including choreoathetosis), sleep disorders, autonomic dysfunction and speech dysfunction (mutism, echolalia).It presents with seizures and movement disorders in young children but typically presents with psychiatric symptoms in adolescents.HSE relapse and HSE-associated NMDAR encephalitis may be clinically similar and can be differentiated by the absence of HSV replication in the CSF and the presence of autoantibodies.Approximately 27% of patients with HSE have been shown to produce NMDAR antibodies within three months.Antibody detection within three weeks of HSE is a risk factor for autoimmune encephalitis.
Autoantibodies were not routinely studied in any of our patients and antibodies were only studied when symptoms appeared.The mean of patients age who developed autoimmune complications presented with movement disorder were 51 months, presented with psychosis and self-mutilation 172 months, which is concordant with the literature in our study.Autoimmune complications developed in four (25%) patients and were observed for an average of 29.5 days after treatment.Autoimmune complications were observed within a shorter time than the adult age group in our study which is similar as reported in other childhood studies[18-20].Autoimmune complications associated with short-term acyclovir treatment were presented in adult series[16], while in our cases, all patients received acyclovir treatment for 21 days.Poor neurodevelopmental outcomes have been reported with a rate of 50% in HSE-related movement disorders.The current data[18-20] confirm that young children choreoathetosis may be accompanied or preceded by refractory seizures or status epilepticus.In our cases, refractory seizures accompanied choreoathetosis in patients 14 and 16.Poor outcomes were observed in 50% of our patients who had resistant epilepsy and motor disability (patients 14, 16).
Children with herpes simplex virus encephalitis have a relapse which rarely presents as a movement disorder, most often choreoathetosis.The anatomic basis for herpes simplex virus encephalitis-associated movement disorders has been poorly understood, because neuroimaging, to date, has not been able to show the direct involvement of the areas of the brain that typically govern such movements.Undetermined antibodies may be presented but can be overlooked when samples are not screened using immunofluorescence on brain sections.Negative testing for autoantibodies during relapsing symptoms post-HSE, therefore, does not exclude an autoimmune cause.Accordingly, treating physicians should always consider immunotherapy in relapsing symptoms post-HSE, even if no specific autoantibodies are found[21].In our study,autoantibodies tests were positive in three patients with NMDARE and negative in the patient who was diagnosed with post-HSE choreoathetosis.
The treatment principles of post-HSE autoimmune complications are: steroids, IVIG and/or plasmapheresis which are the firstline regimens.The second-line regimens are rituximab or cyclophosphamide[25,26].All patients benefited from immunotherapy,and pulse steroid is the first treatment choice, except for one patient who received only IVIG therapy due to negative autoantibodies and possible paraneoplastic syndrome.The prolongation of the immunotherapy was due to the partial resolution of complaints or prevent relapses.We observed that seizures and movement disorders were controlled with immunotherapy.
We believe that immunotherapy should be initiated after detecting autoimmune antibodies simultaneously with CSF analysis in patients with HSE.Treatment should be started early upon recognition of autoimmune complications through follow-up by measuring autoantibody levels and clinical examination results.In our study,there were no findings that would enable early diagnosis or prediction of patients with autoimmune complications, and routine autoantibody analysis might be beneficial.
Poor outcomes were thus evident in patients with older age, lower Glasgow Coma Scale scores and no corticosteroid administration in the acute stage.In a study among adults[22], steroids were administered concurrently with acyclovir and had a positive effect on prognosis.In an animal experiment study[23], there was a significant reduction in the severity of long-term MRI abnormalities in acyclovir/corticosteroid-treated animals.In a pediatric case series of five patients by Genc et al[24], it was reported that the neurologic prognosis was better in patients who were treated with steroids.
There are several limitations in this study.Because the study was retrospective and the viral copy number was not studied, we couldn’t be able to report these results.Future studies with longer followup and a larger number of cases are required to assess the long-term complications and treatment responses.
Autoantibodies should be studied routinely.Treatment should be started early upon recognition of autoimmune complications through follow-up by measuring autoantibody levels and clinical examination results.Patients should be followed closely for autoimmune complications.Randomized controlled studies are needed for the initiation of concomitant immunotherapy with acyclovir in risky cases.However, none of these treatments are prophylactic or curative, motor disability cannot be prevented.Effective prevention and curative treatment modalities are needed to avoid HSE complications.
Conflict of interest statement
The authors declare no competing interests.
Ethical approval
The study was approved by the Medical Faculty Clinical/Human Research Ethics Committee (approval no.HRU.19.05.23) and was conducted according to the Helsinki Declaration principles.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’ contributions
GD?, GB developed the theoretical formalism.GD?, ES, TS studied for data acquisition.GD?, ES and GB contributed to the final version of the manuscript.GD? supervised the project.All authors have approved the final version of the manuscript.
 Asian Pacific Journal of Tropical Medicine2023年5期
Asian Pacific Journal of Tropical Medicine2023年5期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Electrocardiographic changes in dengue fever
- Antibiotic resistance and molecular typing of clinical Staphylococcus aureus isolates from Malaysian military hospital
- Hepatitis B vaccination status and associated factors among health science students
- Faunal richness and checklist of sandflies (Diptera: Pyschodidae) in India