
The relationship between experience of knee pain and physical activity participation: A scoping review of quantitative studies
2023-05-14 09:08:46LuYngPeipeiWngBronwynMcGill
Lu Yng ,Peipei Wng ,Bronwyn McGill ,c,*
a Sydney School of Public Health,University of Sydney,NSW,Australia
b Department of Hematology,Huashan Hospital,Shanghai,China
c Prevention Research Collaboration,Charles Perkins Centre,University of Sydney,NSW,Australia
Keywords: Exercise Knee Long-term conditions Pain Physical activity
ABSTRACT Objectives: Physical activity (PA) in people with knee pain can help to relieve pain and prevent health problems.However,engaging in regular PA is challenging for them due to chronic musculoskeletal pain.An understanding of how the experience of knee pain affects PA is important to minimize the negative effects of knee pain on participation in PA among this population.We examined the quantitative evidence describing the relationship between the experience of knee pain and participation in PA.Methods:We conducted a scoping review based on the PRISMA-ScR process across 27 items and Peters’methodological framework.Searches using keywords were performed in Medline,PsycINFO,CINAHL and Scopus.Results:Nine studies were included in this review.While one study clearly showed that increased knee pain increased PA,four studies indicated that knee pain decreased PA among individuals with knee pain.One study revealed that increased knee pain decreased moderate PA,but no significant difference with light intensity PA.Three studies showed that knee pain had no impact on PA.Moreover,psychological factors (catastrophizing and pain-related activity interference) and certain activities of daily living were risk factors for insufficient PA among people with knee pain.Conclusions:The limited quantitative evidence on the relationship between the experience of knee pain and PA participation highlights a gap in the knowledge base.The review findings found mixed results,with a negative,positive or no relationship between knee pain and levels of PA among individuals with knee pain.The findings also suggest that the relationship can be affected by psychological factors and different levels and types of PA.Therefore,practitioners should consider multi-component interventions which aim to increase PA levels of individuals with knee pain,after considering the above mediating factors.
What is known?
·Previous studies suggest that physical activity in people with knee pain can help to relieve pain and prevent health problems,but only a small proportion are physically active.
·Quantitative evidence investigating the impacts of the experience of knee pain on physical activity participation and the mediating factors has been lacking.
What is new?
·Based on the limited quantitative evidence,our scoping review found mixed results,with a negative,positive or no relationship between knee pain and levels of physical activity among individuals with knee pain.
·Psychological factors (catastrophizing and pain-related activity interference) and different levels and types of physical activity can affect the relationship between experience of knee pain and physical activity participation.
1.Introduction
Knee pain is a common musculoskeletal condition and often negatively impacts lower extremity physical function [1-3].Knee pain affects a large number of people aged 50 years or older globally[4,5].In the United Kingdom,approximately 1 in 4 individuals in this age group experienced knee pain [6-8].Similarly,around 83.2% of Korean female adults with knee osteoarthritis (KOA) suffered from knee pain on the basis of around 40%of Koreans over 50 years of age with KOA [9,10].Although there are a wide range of sources for knee pain,it is largely attributed to the presence of underlying KOA [6-8,11].
KOA is also a serious public health problem [12,13].A study in 2022 showed that the global prevalence of KOA was 16%,the pooled global incidence was 203 per 10,000 person-years,and there were approximately 654.1 million people with KOA aged 40 and older in 2020 around the world [13].
KOA is frequently accompanied by comorbidities (such as cardiovascular disease,obesity,diabetes,hypertension and depression) that can lead to decreased quality of life [9,10,14-17].Two studies conducted in general practices in the United Kingdom and South Korean households demonstrated that a significant number of individuals with KOA are at a greater risk of being diagnosed with two or more diseases[9,18].There is strong evidence that KOA is the 11th highest cause of disability worldwide [19].Furthermore,the economic burden caused by KOA is elevated [20-22].KOA contributed more than $27 billion in health care expenditures in America annually to 2013 [20],which is consistent with Korean data from 2019,indicating observed increases in the economic burden to the Korean health care system[21].Similarly,the annual absenteeism costs caused by KOA in the Dutch workforce are substantial at around €27 million [22].
To avoid knee pain and relevant health and economic burdens,regular physical activity (PA) is widely recommended [23-25].Specifically,being physically active can help to relieve knee pain and prevent these health problems,ultimately improving quality of life for people with knee pain [15,16,26].However,knee pain has been identified as a major barrier to PA participation [27-31].Systematic reviews indicate that knee pain hinders the ability to engage in PA [27,31].Some individuals considered that knee pain was so aversive and stressful that it stopped them from following their previous activity patterns,thus leading to a lower level of PA than before[27].
Given the large number of people affected by knee pain who are physically inactive,it is important to understand how knee pain affects participation in PA.To our knowledge,no reviews have investigated the impact of an individual’s experience of knee pain on PA.Addressing this gap in the literature could encourage the design of improved intervention strategies to promote PA without exacerbating pain,ultimately preventing KOA-related health problems and improving the quality of life for those with KOA.Researchers might prioritize quantitative research for the purpose of investigating the impacts of the experience of knee pain on PA,because research which quantifies the experience of knee pain and PA from the population can provide more reliable and accurate results about the relationship than qualitative research [32,33].Quantitative data can usually be generalized to a larger population,emphasizing large samples that can provide an overview of an area that can reveal patterns and inconsistencies [33].Moreover,the researcher is more objective about the findings of the research using well designed quantitative studies [33].
The purpose of this scoping review is therefore to explore the quantitative evidence about the relationship between the experience of knee pain and PA participation.To achieve this,we addressed two objectives:to determine how the experience of knee pain affect PA participation among adults with chronic knee pain;and to determine the factors that affect the relationship between the experience of knee pain and PA participation.
2.Methods
This research aims to provide a broad overview of the relationship between the experience of knee pain and PA participation.Scoping reviews examine emerging evidence on a topic which has not been comprehensively reviewed[27].We therefore conducted a scoping review to examine the extent,range,and nature of evidence on the impacts of experience of knee pain and PA participation [28,29].The scoping review followed the PRISMA-ScR process across 27 items [34] and scoping review guidelines from Peters [35,36].The final protocol is available (Appendix A).
2.1.Eligibility criteria,study selection and information sources
The researcher (L.Y.) defined the search syntax and key terms for the scoping review,which was tested,discussed and agreed by all researchers on the team,prior to database searches (Table 1).
Inclusion and exclusion criteria were defined using the same process,with the research team focusing on identifying quantitative research that investigated the impacts of experience of knee pain on PA participation (Table 2).Electronic searches were run in the databases on 13 July 2022,with no limitation to date.
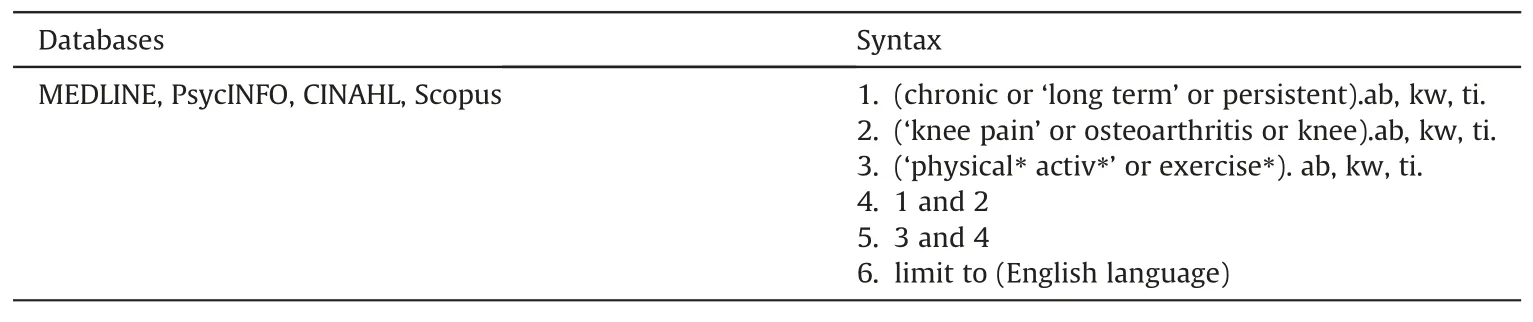
Table 1 Information sources and search syntax.

Table 2 Selection of sources of evidence.
2.2.Data items,charting process and results synthesis
Title,abstract and full text screening against keywords,inclusion and exclusion criteria was undertaken by two reviewers(L.Y.,P.W.).Both researchers met to discuss outcomes and reach consensus on the final articles to be included for full text review.Any conflicts were solved by a third reviewer (B.M.).Cohen’s Kappa statistics were calculated to test inter-rater reliability [35].Search results from all datasets were combined and imported into Covidence(www.covidence.org).More details on the search results are provided in Appendix A.
A data charting form was created by the first author to extract data relevant to our research question.The data charting form was trialed by the three authors,and modifications were made to ensure that the information would address the research question.Data were extracted for reference,country,study quality,study aim,study type,study design,setting,timing of data collection,information on study populations,exposure &measurement,outcome&measurement,and main findings/conclusions (Appendix B).
A narrative synthesis was conducted to synthesize and report the results [37].A single reviewer (L.Y.) performed tabulation,textual description,grouping and clustering,and conceptual mapping of the data,which was then discussed among the three reviewers and any differences in opinion resolved through discussion.Data synthesis involved examination of the data extraction table to determine the presence of dominant groups or clusters of characteristics,by which the subsequent synthesis could be organized.
To draw conclusions not based on potential bias,critical appraisal of study quality was conducted [38,39],which used Joanna Briggs Institute (JBI) methodology for scoping reviews for evaluation [35,40].Two reviewers (L.Y.,P.W.) independently appraised the methodological quality of included studies using JBI Critical Appraisal Checklist appropriate to each study type [37,41],and a third reviewer (B.M.) resolved any disagreement.Each checklist consists of 8-11 items which are classified into 4 categories: “Yes”,“Unclear”,“No” and “Not applicable”.For assessing the quality of the studies,a score of three points was assigned to the“Yes”category,one point to“Unclear”,and zero points to“No”,and“Not applicable”was removed.Based on the final score,the quality was grouped according to high quality (≥66%),medium quality(34%-65%)and low quality(≤33%)[42].Studies were not excluded according to quality given that the aims of a scoping review are to identify the nature,range and extent of research[43].
3.Results
3.1.Literature search
The search yielded 1,429 articles and resulted in nine studies being included in the review (Fig.1).One study [44] was not included as the full text could not be obtained due to resource limitations.
3.2.Characteristics of included articles
All nine studies were published between March 2007 and March 2022[30,43,45-51].Five studies took place in community settings[45,47-49,51],two in clinic settings including general practice and rheumatology clinics [30,50],one in both community and clinic settings [46] and one in both the community and a health care centre[43].All studies were carried out in high-income countries.Six studies were conducted in the United States[43,45,47-50],one each in Japan,the Netherlands and Germany[30,46,51],and one in six European countries [51].Of the articles,seven consisted of secondary data analysis [30,43,45,47,48,50,51] and the other two were primary studies [46,49].All studies used a cross-sectional study design [30,43,45-50],with the exception of one which was a prospective cohort study [51].Three studies used data collected over a period of more than a one-year period[48-50]and two used data collected over a period of 1 week or less[45,47].The European study used six data sets with data collected over 12-18 months[51],and the other only showed the timing of data collection on PA but did not show that on knee pain[46].The remaining two did not specify the time frames of their data collection[30,43].More details on the characteristics of included articles,study populations,exposure and outcome measures,the relationship,mediating factors,and quality assessment are shown in Table 3 and Appendix B.
3.3.Information on study populations
The median sample size across all studies was 350 per study,ranging from 143 to 1,874.Over half of all participants were women and the median age of all participants was 66 years.In terms of participants’ ethnicity,six studies reported a predominance of Caucasians,ranging from 73.7% to 90.0% [43,45,47-50].Three studies did not report the ethnicity of participants [30,46,51].
Four studies focused on individuals with or at high risk for KOA and chronic knee pain [43,47,48,50].Three studies focused on individuals with KOA or at high risk for KOA without reporting the details of knee pain[45,46,49].The remaining two studies focused on individuals with knee and hip osteoarthritis[30,51].In terms of comorbidities,only two studies reported that the percentages of comorbidity/no comorbidity were 30% and 59%,respectively[48,49].Obesity was considered in seven studies [30,45-49,51].The mean body mass index(BMI)ranged from 28.3 to 31.2 kg/m2in four studies (44%) [30,47,49,51],one study only focused on participants with overweight and obesity [45],and one study included 35% of participants with obesity [48].By contrast,in the study conducted by Fukutani and colleagues,the mean BMI of participants in both early and severe KOA groups was below 25.5 kg/m2[46].To reduce effects of other diseases on the relationship,researchers in the five studies excluded persons with diseases related to rheumatism (such as rheumatoid arthritis,fibromyalgia) and/or physical inactivity [43,46,47,49,50].
The majority of studies (n=7) did not provide information on medication use which affected the relationship between experience of knee pain and PA participation [30,43,45,48-51].Two studies considered the effects of the medication use on this relationship,by excluding persons with medical conditions causing pain from the study [46,47].With regard to knee surgery,six studies excluded individuals who had or needed surgery[43,46-50].The remaining three studies did not report any treatment which participants had or had not received before the research [30,45,51];and there were no treatments during the research among all participants [30,43,45-51].
3.4.Tools used to measure knee pain
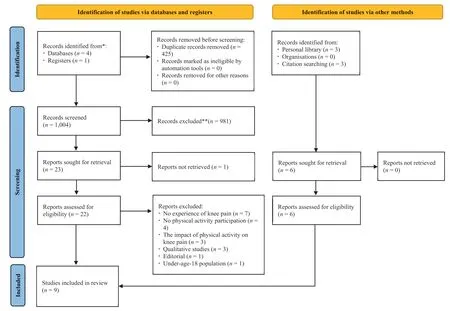
Fig.1.PRISMA 2020 flow diagram for the study.
Participants’ experiences of knee pain were assessed by selfreported questionnaires in all papers [30,43,45-51].Knee pain measurements exhibited heterogeneity with a total of seven different measures used to operationalize the construct.The most commonly used measure was the Western Ontario McMasters Universities Osteoarthritis Index (WOMAC) [45,51].With the exception of one study which did not report the measurement of knee pain [30],the remaining studies used different scales which included Brief Pain Inventory (BPI) [47],the Coping Strategies Questionnaire [50],the Japanese Knee Osteoarthritis Measure(JKOM) [46],the Knee Injury and Osteoarthritis Outcome Score(KOOS) [43],the Intermittent and Constant Osteoarthritis Pain(ICOAP) [48],and Visual Analog Scale (VAS) [49].
3.5.Tools used to measure physical activity participation
Different types of accelerometers were used to record activity counts in three studies [47,48,50],namely ActiGraph accelerometers,the Kenx Lifecorder uniaxial accelerometer and the Actiwatch Score accelerometer.Pedometers were used in one further study[46].Besides objective assessments to measure the levels of PA participation,three studies used self-reported questionnaires[30,45,51].In addition to accelerometers,Chemlo et al.[45] used self-reported Physical Activity Scale for the Elderly (PASE).Rosemann et al.[30] used short form of the International Physical Activity Questionnaire(IPAQ).Schoor et al.[51]used the Longitudinal Aging Study Amsterdam (LASA) Physical Activity Questionnaire.
3.6.The impacts of the experience of knee pain on physical activity
Of the small number of quantitative studies(n=9),the findings indicated mixed results on the relationship between experience of knee pain and PA participation.Four studies indicated a negative association between knee pain and PA (increased knee pain decreased PA) [30,43,46,50].One study indicated that increased knee pain related to decreased moderate PA,but no significant difference with light intensity PA [48].Another study reported specifically on the moderating effects of pain on PA indicating the positive relationship between experience of knee pain and PA participation[47].A further three studies found that knee pain had little to no impact on PA [45,49,51].
Four studies demonstrated a negative association between knee pain and PA [30,43,46,50],and one showed a negative association between knee pain and moderate PA [48].Gunn and colleagues found that over half of participants with KOA did not make any unnecessary movement due to knee pain,which suggests that knee pain can cause low levels of PA[43].Zhaoyang,Martire and Darnall found that study participants with a higher severity of knee pain engaged in a lower level of PA[50].The results of these two studies were consistent with a Japanese paper,showing that participants were less likely to engage in PA when they experienced knee pain during activities of daily living[46].Similarly,Rosemann et al.[30]demonstrated that patients’pain limited PA(P<0.001).It is worth noting that Song et al.[48] found different directions in the relationship between experience of knee pain and two intensity levels of PA participation (light or moderate intensity PA).On the one hand,consistent with the negative association found in the five studies,there was a statistically significant trend between increasing pain levels and decreased time spend in moderate PA(from 72 min/week among those with no pain to 52 min/week among those with constant pain,P=0.03)[48].Specifically,study participants with constant pain spent 26%less time in moderate PA than those without knee pain,and those with higher intermittent pain spent 19% less time in moderate activity than individuals reporting no knee pain [48].On the other hand,Song et al.[48]found that time spent in light activity did not differ statistically among the four knee pain groups(no pain,lower intermittent pain,higher intermittent pain and any constant pain),and therefore worse knee pain had no significant relationship with light intensity PA.

One study demonstrated an association between knee pain and PA participation in the context of moderating factors[47].Murphy et al.[47]found that increased pain was associated with increased PA,but only in the first part of the day when people tend to be more active.While this relationship was not causal,there was a possible moderating effect of pain-related activity interference,where people with low pain-related activity interference may persist with activities,despite the possibility that the activity may increase their pain [47].
An additional three studies revealed that knee pain did not affect PA [45,49,51].One study demonstrated no significant correlation between knee pain and PA levels [49].Among male participants,12.9% with moderate-to-severe pain met recommended PA guidelines compared with 10.9% without pain (P=0.74);and among female participants,PA guidelines were met by 6.7% with moderate-to-severe pain and by 11%without pain(P=0.40)[49].In addition,Chmelo et al.[45] indicated that there were no statistically significant differences between mild knee pain and light(P=0.58)or moderate-to-vigorous PA(P=0.07).Similarly,Schoor et al.[51]found no meaningful differences on the PA level between persons having lower limb osteoarthritis (LLOA) with and without persistent severe pain (P=0.36).
3.7.Factors that might influence the relationship between knee pain and physical activity
Three studies investigated the mediating influence of other variables in the relationship between the experience of knee pain and PA levels[46,47,50].These studies explored how psychological factors [47,50] and activities of daily living [46] affected the relationship between knee pain and PA.
A negative cognitive-emotional response,or catastrophizing in relation to knee pain was associated with a low level of PA among people with KOA[50].Zhaoyang,Martire and Darnall reflected that pain catastrophizing in the morning could significantly reduce the hours that people with KOA spent in moderate-to-vigorous PA on the same day[50].For individuals with one unit higher than usual catastrophic thinking about their knee pain in the morning,they spent 3.08 min less in moderate-to-vigorous PA (P=0.006) [50].Engaging in less moderate-to-vigorous PA could further lead to greater pain catastrophizing the next morning,creating a negative cycle(P=0.002)[50].Regarding pain-related activity interference(the relationship between pain levels and interference with engagement in physical activities),people with KOA with low painrelated interference were more likely to participate in PA without being affected by knee pain earlier in the day[47].Compared with those with the medium or high levels of pain-related activity interference,people with KOA with low pain-related activity interference had more positive attitudes towards their momentary pain severity and therefore be more willing to take part in PA earlier in the day [47].In short,psychological factors such as catastrophizing and pain-related interference affect the relationship between knee pain and PA.
In addition to pain catastrophizing and pain-related interference,activities of daily living contributed to the impact of knee pain on PA participation,making people feel more pain and therefore less likely to engage in PA[46].For individuals with early KOA,the more knee pain they experienced while ascending stairs,the lower their PA levels were (75th percentile regression coefficient=-1,033.7,95%CI-1,924.27 to-141.73,P=0.018)[46].For those with severe KOA,the more knee pain they experienced while walking on a flat surface and bending to the floor,or standing up,the lower their PA was(-1,850.87,95%CI-3,474.12 to-227.63,P=0.026 and -2,640.35,95% CI -4,617.39 to -663.32,P=0.010)[46].
3.8.Quality assessment
All included studies were found to be of high quality,with the exception of one study reported to be of medium quality(Appendix C).Risk of bias primarily arose from aspects regarding measures and the criteria for sample.For example,self-reported questionnaires for measuring knee pain levels may have led to high risk of measurement bias in all reviewed studies [30,43,45-51].Nonreporting of response rates may also have had significant selection bias [43,45,46,48,49,51].In addition,a lack of information on participants (e.g.medication use for relieving knee pain,previous knee replacements) in two studies may have affected the results and conclusions [43,45].
4.Discussion
Our scoping review identified a small number (n=9) of quantitative studies which provide an overview of the current literature which investigates the relationship between the experience of knee pain and PA participation.The findings of the review will contribute to filling a gap in the literature on how the experience of knee pain can affect PA participation of individuals with knee pain.
We found that the existing body of research has overwhelmingly focused on exploring how to reduce the ‘negative’impacts of knee pain on PA participation in practice.This is probably due to the numerous researchers who inferred that knee pain can lead to physical inactivity from the weak evidence (such as from papers focused on individuals with low back pain or arthritis or chronic pain)[52-55].This may reflect that many researchers so far have assumed that knee pain can lead to physical inactivity without robust evidence,and that they are more interested in tackling physical inactivity than exploring how the experience of knee pain affects PA participation.
4.1.Study population and the characteristics of the included articles
Given that over 70% of participants in our review (6/9) were Caucasian,there is a need to conduct more research investigating the statistical relationship between the experience of knee pain and PA participation among other ethnicity groups.In addition,more primary quantitative studies need to be conducted in middle-and low-income countries,as our scoping review only identified nine papers investigating the relationship between experience of knee pain and PA in high-income countries,seven of which were secondary data analysis.Furthermore,in order to understand the directionality of the relationship between experience of knee pain and PA,longitudinal studies are needed as the majority of reviewed studies (8/9) used cross-sectional study designs to explore the relationship [56].
4.2.The mixed findings of the relationship between experience of knee pain and physical activity
The present study identified mixed findings of the statistical relationship between experience of knee pain and PA participation.Consistent with previous studies which indicated that pain has a complex association with PA [54,55,57-60],the synthesis of the findings of these studies was mixed with a negative,nonsignificant or positive relationship between knee pain and the levels of PA.This inconsistency may be explained by four factors(differences in sample and objective,study design and measurement).As noted,Chmelo et al.[45] revealed a nonsignificant relationship between experience of knee pain and PA participation.One of the plausible explanations may be,unlike any other included studies,this study included persons with a sedentary lifestyle,which may have affected the directionality in the relationship.Additional three studies also found no association between the experience of knee pain and PA participation.The inconsistency of directionality in the relationship may be due to the effects of comorbidity among participants.In our scoping review,we found that two of the three studies showing a non-significant association were the only studies which regarded percentages of comorbidity (30%) or no comorbidity (59%) as a major covariate.
In terms of the different objectives of studies in our scoping review,Murphy et al.[47]aimed to explore the mediating effects on the relationship between symptoms (e.g.knee pain) and PA,and did not focus on the directionality of the relationship,thus potentially leading to different findings.Another possibility for the mixed findings relates to the predominance of cross-sectional studies.As most selected studies were cross-sectional,measurement bias of cross-sectional studies may have led to mixed findings [61].Specifically,participation in PA among non-responders might differ from responders,leading to the mixed findings in this review[62].Lastly,different results of the relationship might be partly due to the exposure and outcome measurements.The levels of knee pain and PA might be over-or under-estimated in all selected studies due to an over-reliance on self-report measures[58].Self-reporting knee pain levels(92%)are susceptible to response and recall bias in most studies (92%) [58].Similarly,one third of studies only used questionnaires to measure PA levels,which may also have led to response and recall bias [58].Objective measurements of PA may have affected the conclusion on the relationship between experience of knee pain and PA participation [61].As the majority of studies used accelerometers,pedometers or monitors to measure PA levels (58%),participants were aware that their daily PA was being recorded[61].There is evidence that participants may change daily exercise habits when they know it is being recorded,possibly resulting in under-or over-estimation of PA [61].Collectively,the measures for keen pain and PA might have led to the mixed findings of the relationship and need to be developed to investigate the impacts of knee pain on PA participation.
4.3.Mediating factors
Our findings also suggest the mediating influence of psychological factors such as catastrophizing and pain-related interference which may improve our understanding of the relationship between pain and PA.Moreover,our review demonstrated that different levels and types of PA(such as ascending stairs in persons with early KOA,walking on a flat surface or bending to the floor or standing up in persons with severe KOA) also affect the impact of knee pain on PA participation.As psychological factors,and different levels and types of PA affect the relationship between the experience of knee pain and PA participation,our findings suggest that future research should consider multi-component interventions which focus on supporting individuals to increase their levels of PA,giving consideration to these factors related to psychology and different levels and types of PA.
4.4.Implications
The narrative synthesis found that knee pain did not influence light-intensity PA,but negatively influenced moderate-intensity PA among people with KOA,which is consistent with the findings in a mixed methods study indicating that gentle activity was favored over more vigorous exercise by people with knee and hip osteoarthritis[63],and that this population would be more willing to take part in low-impact activities[64].Therefore,light-intensity and low-impact PA need to be considered when planning appropriate PA for those with knee pain [63,64].Furthermore,different types of activity may affect participation in PA in the context of knee pain.
For individuals with early KOA,knee pain caused by ascending stairs negatively affected their PA levels.For those with severe KOA,their PA levels can be negatively affected by knee pain they experienced while walking on a flat surface or bending to the floor or standing up.Therefore,consideration needs to be given to tailor the type of PA which is suitable for individuals with knee pain and different levels of KOA to improve their PA participation.
In addition to individually tailored activities,individual preference has been reported as important for improving PA levels among adults with knee pain [63,65,66].Loew et al.[65] demonstrated that individuals with KOA assigned to a preferred walking program showed greater adherence to the program over time,compared with those who were assigned to a non-preferred one.It is possible that personal preference may help individuals with KOA complete exercise within the limit of their pain [63],avoiding or modifying previous activities which were painful and resulted in symptoms[63].
Our findings also suggest that catastrophizing and pain-related interference negatively affect participation in PA in the morning,and therefore morning hours might be an important period to help more individuals with knee pain to engage in psychological interventions.In order to reduce physical inactivity caused by the two psychological factors in the morning,morning self-efficacy might be highlighted [67].Zhaoyang et al.[67] have revealed that when people with knee pain were more confident than usual in their ability to be active throughout the day,they took more steps and spent more time in moderate-intensity activity that day.Furthermore,pain catastrophizing has been widely considered as a modifiable factor that negatively affects participation in PA[68-70].Greater pain catastrophizing is associated with lower PA levels among people with KOA[68-70].However,findings related to knee pain are inconsistent [69].Contrary to the findings in our review and two additional studies(pain catastrophizing intensified pain) [70,71],another study suggested that pain catastrophizing was associated with PA after adjusting for pain levels,which means that one’s personal attitude toward pain is not related to pain severity,but related to PA[69].Collectively,despite the uncertainty about the relationship between pain catastrophizing and pain severity,strategies to improve pain catastrophizing might be useful in enhancing PA participation.
4.5.Strengths and limitations
Our study provides useful information on the extent (size),range (variety) and nature (characteristics) of the evidence on the statistical relationship between experience of knee pain and PA.We identified limited evidence on the statistical relationship between the experience of knee pain and PA participation,which highlights a lack of comprehensive research on this topic and demonstrates a gap in the knowledge base.Although critical appraisal is not essential in a scoping review[34,72],this study is strengthened by the critical appraisal of included studies and the statistical measure of inter-rater reliability [73].
A few limitations to our scoping review should be considered.Our scoping review provides an overview of the evidence published in English,and relevant information published in other languages may therefore have been overlooked [61].Future reviews on this topic should focus on research published in a broad range of languages.Our scoping review focused on quantitative evidence.While we have provided an overview of the literature available,qualitative and mixed methods data would provide a more comprehensive and nuanced understanding of the relationship between experience of knee pain and PA participation[27,65,66,68,74].There is evidence that qualitative studies also demonstrate a positive or negative relationship,identifying that the experience of pain may decrease or increase PA among individuals with KOA [66,68,74].Additionally,a mixed methods study indicated that although fewer people with knee pain were physically active than those without knee pain,the difference was not statistically significant [65].While it is also challenging to determine the relationship between experience of knee pain and PA participation from the research on qualitative and mixed methods studies,future evidence reviews should include these studies in addition to quantitative studies.
5.Conclusion
The findings in this scoping review have public health significance.Although a large number of people suffer from knee pain,and PA is widely recognized as one of the most effective interventions for improving the health conditions of those with knee pain[12,23-25],a large proportion are still physically inactive and spend more time in sedentary behavior than the general population[75,76].In response to insufficient PA among individuals with knee pain,our findings identified limited literature on how the experiences of knee pain impact on PA,but can contribute to beginning to better understand this topic.
Funding
No funding to declare.
CRediT authorship contribution statement
Lu Yang:Methodology,Validation,Formal analysis,Investigation,Resources,Data curation,Writing -original draft,Writing -review &editing,Visualization,Project administration.Peipei Wang:Methodology,Validation,Formal analysis,Investigation,Resources,Data curation,Writing-review&editing,Visualization.Bronwyn McGill:Conceptualization,Methodology,Validation,Formal analysis,Investigation,Resources,Data curation,Writingreview &editing,Visualization,Supervision,Project administration.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of competing interest
We have declared no conflict of interest.
Acknowledgements
We would like to express our gratitude to Associate Professor Anne Grunseit for guidance with the conceptualization of this review.
Appendices.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.03.010.
 International Journal of Nursing Sciences2023年2期
International Journal of Nursing Sciences2023年2期
- International Journal of Nursing Sciences的其它文章
- COVID-19 pandemic in long-term care: An international perspective for policy considerations
- 2023 年中華護理雜志社系列中文期刊專題報道計劃
- 歡迎訂閱2023 年《國際護理科學(xué)(英文)》
- 學(xué)術(shù)網(wǎng)站集萃
- Research hotspots and theme trends in post-traumatic growth: A coword analysis based on keywords
- Predictive factors based on the health belief model on cancerscreening behaviour in first degree relatives of patients with Lynch syndrome-associated colorectal cancer