
Management of procedural pain in the intensive care unit
2022-03-15 11:59:18NaNaGuoHongLiangWangMingYanZhaoJianGuoLiHaiTaoLiuTingXinZhangXinYuZhangYiJunChuKaiJiangYuChangSongWang
World Journal of Clinical Cases 2022年5期
lNTRODUCTlON
Pain is a common experience for inpatients,and intensive care unit(ICU)patients undergo more pain than other departmental patients,with an incidence of 50% at rest and up to 80% during common care procedures[1].The inducing factors of pain in the ICU include primary disease,various monitoring devices,treatment,long-term bed rest,and environmental and psychological factors[2].In terms of its duration,pain in the ICU is divided into persistent pain(with inducing factors including mechanical ventilation,surgical incision,)and transient pain(with inducing factors including arteriovenous puncture,abdominocentesis,).At present,the management of persistent pain in ICU patients has attracted considerable attention,and there are many related clinical studies[3-5]and guidelines[6,7].However,the management of transient pain caused by certain ICU procedures has not received sufficient attention.In 2018,although the PADIS guidelines[7]and "The Guidelines for the Management of Pain,Agitation in Adult Patients in the Intensive Care Unit"[2]refer to the prevalence of pain in ICU patients and recommend pain management and sedation to reduce patient discomfort,there are no specific recommendations for managing pain caused by procedures performed in the ICU.Therefore,the purpose of this article is to review the different management strategies for procedural pain in the ICU.
CLASSlFlCATlON OF PROCEDURAL PAlN lN THE lCU
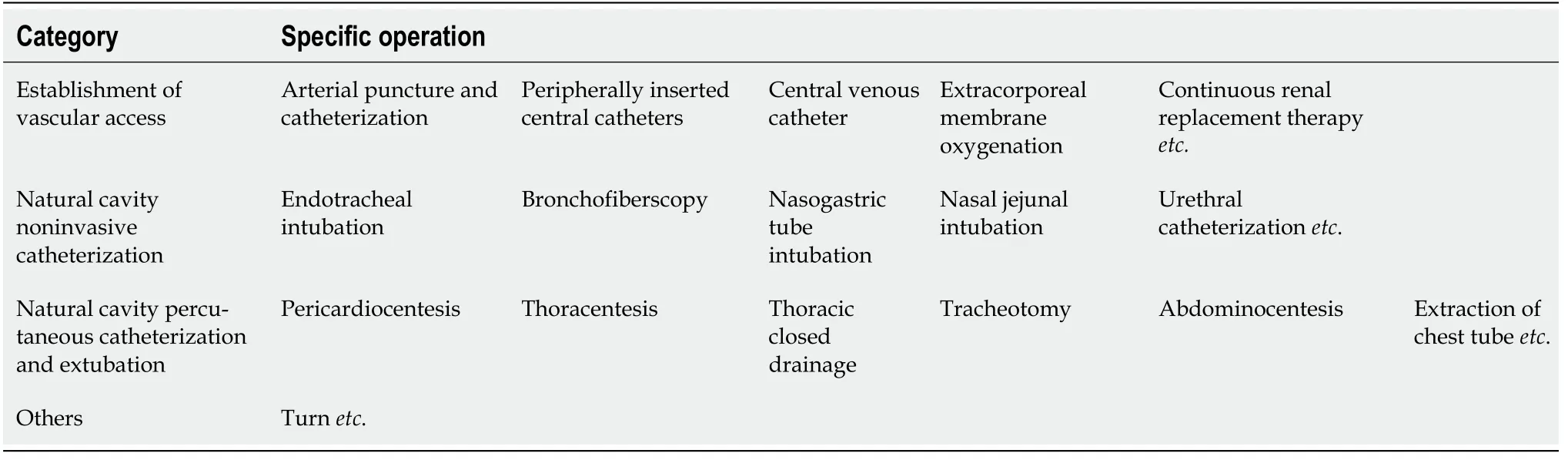
Due to the severity and complexity of diseases in the ICU,various procedures are performed for monitoring,treatment,nursing care and other reasons.According to the procedural purposes,we defined the source of procedural pain into the following four categories:(1)Establishment of vascular access;(2)Noninvasive catheterization of a natural lumen;(3)Percutaneous catheterization and extubation of a natural lumen;and(4)Other procedures(Table 1).Although the above classifications are distinguished for operational purposes,the causes of each type of procedural pain have similar physiological anatomical foundations.
MANAGEMENT OF DlFFERENT CATEGORlES OF PROCEDURAL PAlN
In the past decade,the prevention and treatment concepts of pain,anxiety,and delirium have been updated:treatment based on pain management is emphasized,focusing on early intervention and paying more attention to patient-centered humanistic care while minimizing the side effects of analgesic and sedative drugs[6,8,9]."The Guidelines for the Management of Pain,Agitation in Adult Patients in the Intensive Care Unit" recommend the preadministration of analgesics or nonpharmaco-logical interventions to relieve pain before procedures that may cause pain[2].
The generation of pain involves both physiological and psychological factors.At present,clinical pain management includes pharmacological and nonpharmacological treatments.These drugs include opioid analgesics,nonopioid analgesics,nonsteroidal anti-inflammatory drugs(NSAIDs),and local anesthetics.Nonpharmacological pain management,including hypnosis and distraction by virtual reality,has been used as an adjunct for procedural pain management in ICUs.To date,there is not enough evidence to support the value of nonpharmacological pain management in ICUs[10].Therefore,this review mainly compares the existing pain management approaches from the perspective of drug analgesia according to the different types of procedural pain mentioned above.
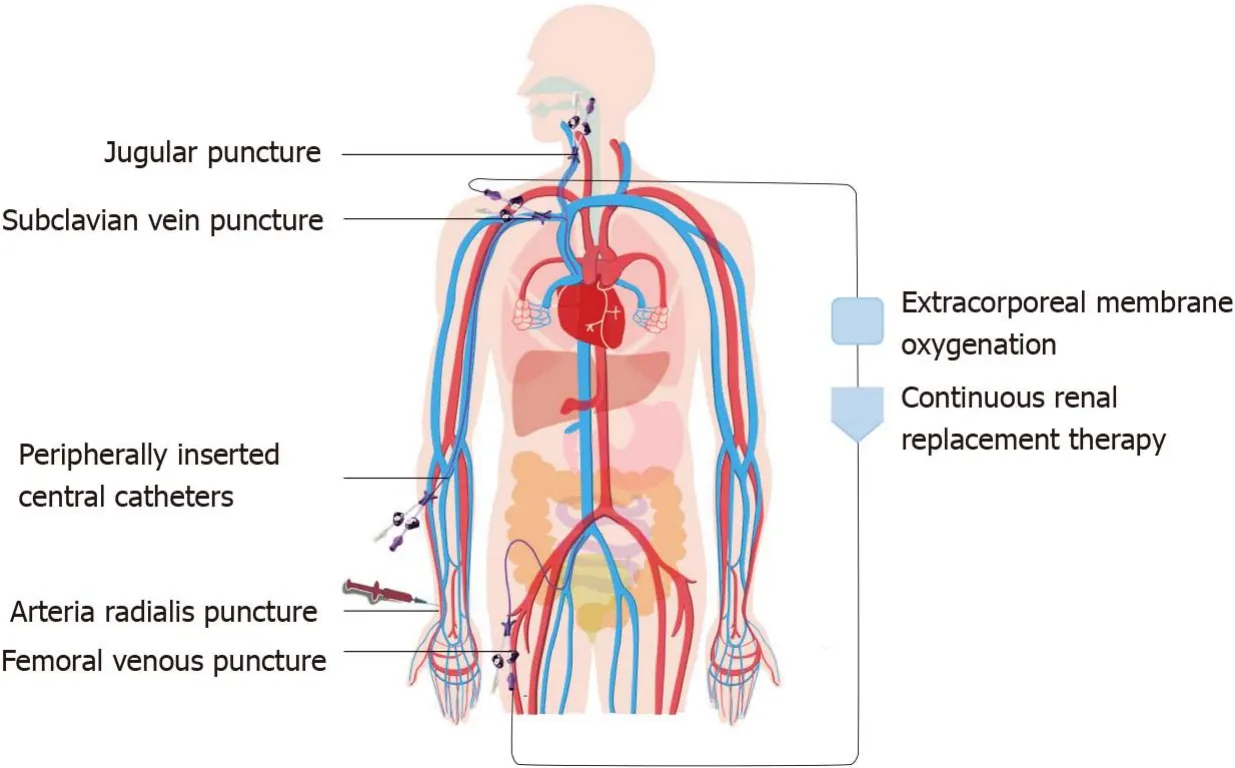
MANAGEMENT OF PAlN CAUSED BY THE ESTABLlSHMENT OF VASCULAR ACCESS
Establishing vascular access is an essential operation in the ICU(Figure 1).For example,arterial puncture and catheterization can enable blood gas analysis and continuous arterial pressure monitoring,and central venous catheters(CVCs)and peripherally inserted central catheters(PICCs)can facilitate central venous pressure monitoring and the rapid administration of liquid and vasoactive drugs.Extracorporeal membrane oxygenation(ECMO)and continuous renal replacement therapy(CRRT)are important organ support methods in the ICU.Both procedures require deep venous catheterization to establish extracorporeal circulation.Improving the patient's oxygenation and excreting metabolic waste from the blood saves valuable time.
There are few pain management studies on thoracentesis and abdominocentesis.The traditional pain management method is local lidocaine infiltration anesthesia,which can provide effective analgesic effects.However,short-term pain management and sedation combined with local infiltration anesthesia may be a better choice,and we expect more clinical studies to confirm this option.The management of pain caused by natural cavity percutaneous catheterization and extubation is shown in Table 4.
She need not have worried. The moor seemed to welcome her back like a long-lost friend and her spirits rose. Taking a deep breath of the clear air, Maggie deftly8 took a bag from her pocket and started to pick, stopping every now and then to straighten her back and enjoy the familiar view. With stained fingers and scratched hands to show for her efforts, the bag slowly filled with the dark, plump fruit.
Pain management during arterial puncture and catheterization and PICCs
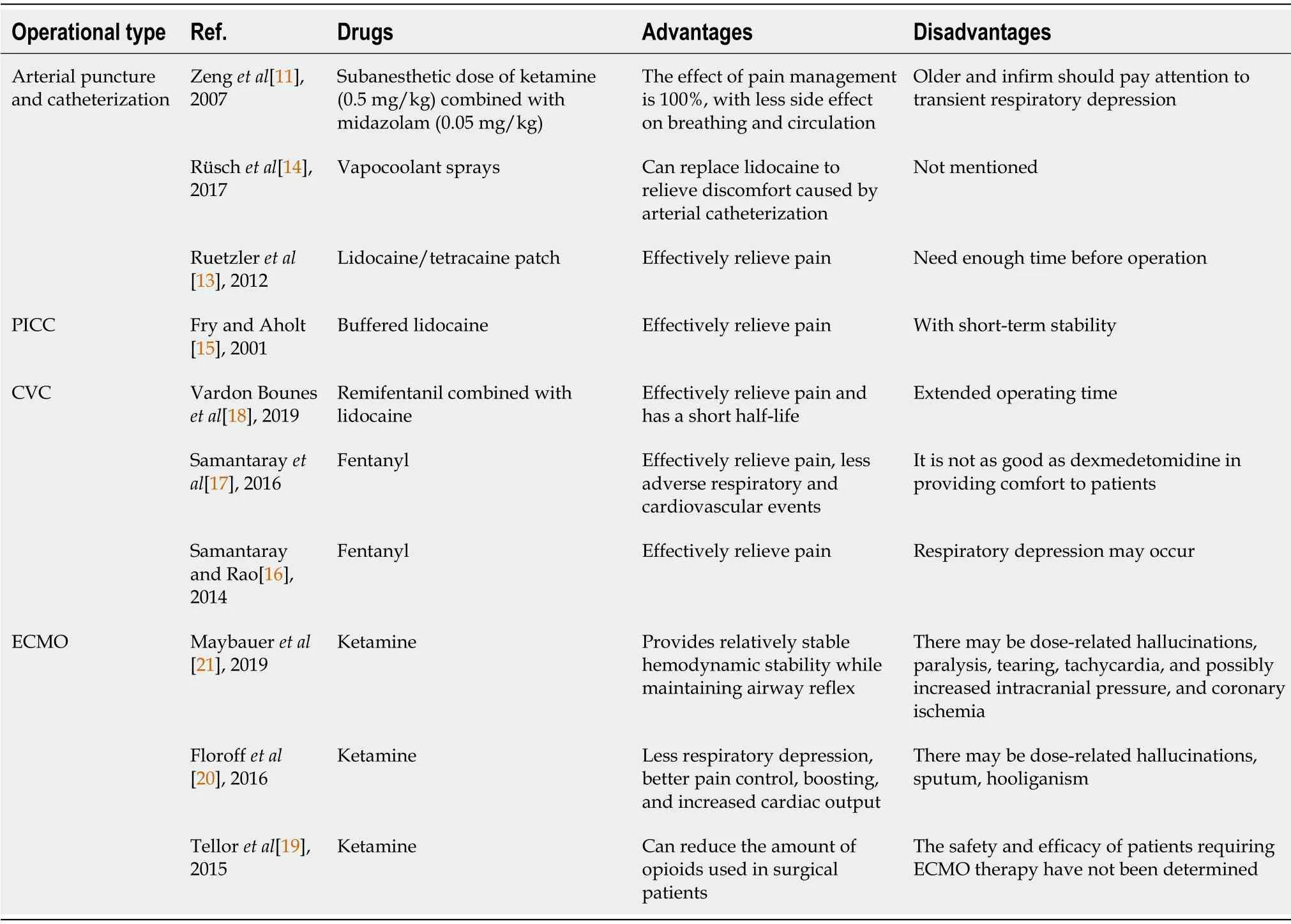
There are few studies on arterial puncture and catheterization or on PICCs with general anesthesia as pain management methods.Zeng[11]found that a subanesthetic dose of ketamine(0.5 mg/kg)combined with midazolam(0.05 mg/kg)for arterial puncture has good analgesic and sedative effects,and most patients can awaken within 5 min to 8 min.When adopting this method,local infiltration anesthesia is not needed,and swelling of the puncture site during local anesthesia is avoided,which is beneficial to improving the success rate of puncture.This method has little effect on the patient's breathing and circulation,but for individuals who are elderly and infirm,it is still necessary to pay attention to transient respiratory depression.Because of the side effects of ketamine on pulmonary arterial pressure and intracranial pressure,patients with pulmonary hypertension or intracranial hypertension should be treated with caution[11].
The next day, T. J. was very active in all the sessions. By the end of the retreat, he had joined the Homeless Project team. He knew something about poverty, hunger and hopelessness. The other students on the team were impressed with his passionate12 concern and ideas. They elected T. J. co-chairman of the team. The student council president would be taking his instruction from T. J. Ware.
Topical anesthesia with different types or formulations of local anesthetics has been used to relieve pain caused by arterial puncture and catheterization and by PICCs in an increasing number of studies.Although topical anesthesia does not cause stabbing pain or local anesthetic poisoning,its anesthetic effect needs to be confirmed by more clinical studies.
Pain management of central venous catheterization
Mechanical ventilation is an important means of respiratory support for critically ill patients.The clinical application guidelines for mechanical ventilation clearly suggest that patients who cannot have their artificial airways removed in the short term should be selected for replacement with tracheotomy as soon as possible[36].A 2010 study showed that compared with tracheal intubation,tracheotomy may increase survival rates in mechanical ventilation patients.However,during tracheotomy,some patients are conscious and experience a certain fear of the procedure.Therefore,appropriate preoperative pain management and sedation are inevitable[37].
The pain management of CVC placement is mostly focused on the intravenous administration of opioid analgesics(remifentanil,fentanyl)combined with lidocaine local infiltration,which can achieve a good analgesic effect while keeping patients awake.Although general anesthesia is more comfortable than local anesthesia,respiratory and circulatory inhibition by general anesthesia cannot be ignored.
Pain management of ECMO
The essence of ECMO is an improved artificial heart-lung machine that can be used for both extracorporeal respiratory support and cardiac support.There is currently no independent study on pain management during the establishment of extracorporeal circulation for ECMO.However,some studies have focused on pain management after extracorporeal circulation establishment.
Two recent case studies and one review suggest that ketamine infusion can be used as an analgesic for ECMO patients,reducing sedatives and opioid doses without changing the Richmond Agitation and Sedation Scale(RASS)score[19-21].Based on the above findings,ketamine combined with local lidocaine infiltration may be an option for analgesia in ECMO patients during the establishment of extracorporeal circulation.
Pain management for CRRT
There is no independent study on the pain management of extracorporeal circulation establishment before CRRT.Mostly,these cases involve renal insufficiency in patients with CRRT.The choice of pain management should avoid nephrotoxic drugs such as tramadol and NSAIDs and may be patterned after pain management for CVC.The management of pain caused by establishing different types of vascular access is shown in Table 2.
In addition to the management of procedural pain caused by the establishment of vascular access,we should also pay attention to improving the success rate of vascular access and avoiding repeated procedures that cause patients more pain.A large number of studies have confirmed that ultrasound guidance in arterial puncture,PICCs and CVCs can not only improve the success rate of puncture but also reduce the incidence of adverse events and improve the satisfaction and comfort of patients[22,23].Moreover,bedside ultrasound can also identify malpositioning of the CVC and pneumothorax faster than an X-ray examination[24,25].
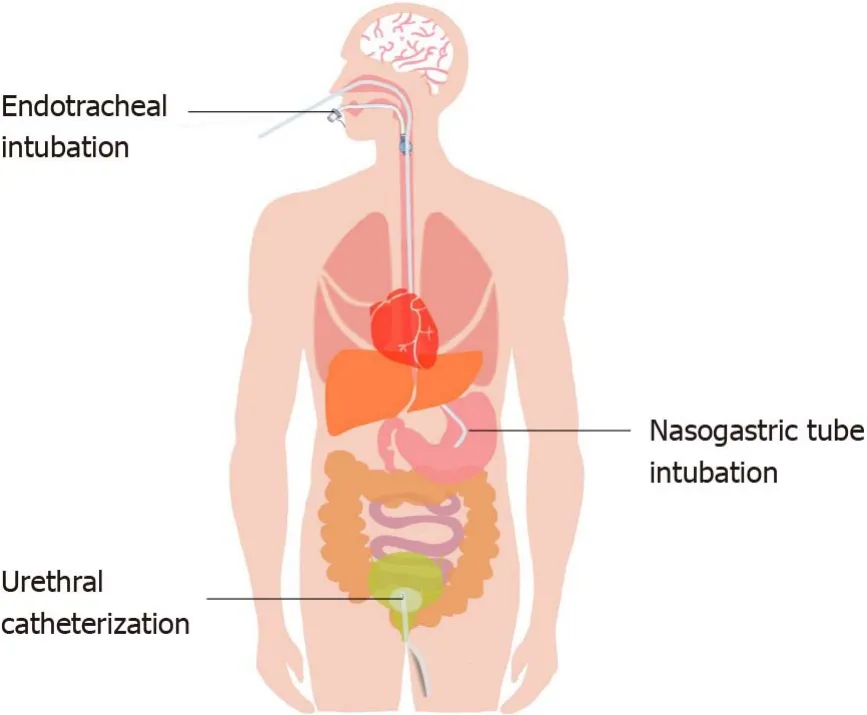
MANAGEMENT OF PAlN CAUSED BY NONlNVASlVE CATHETERlZATlON THROUGH A NATURAL CAVlTY
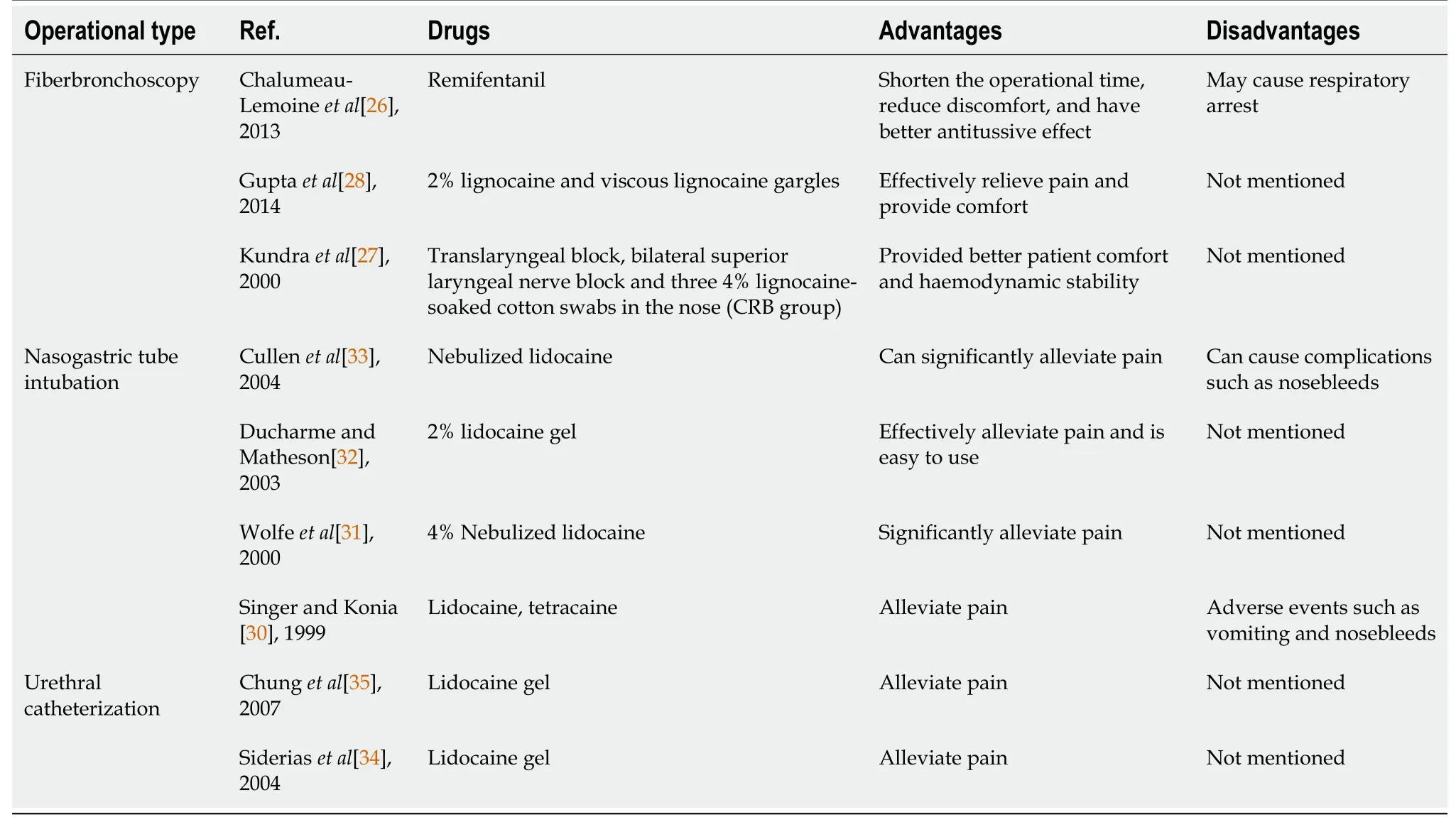
Natural cavities are channels that connect the inside and outside of the human body,and they are sensitive and highly reactive.When a fiberoptic bronchoscope,stomach tube or urinary catheter enters a natural cavity,the device stimulates the mucous membrane,causing discomfort or even pain(Figure 2).Therefore,proper pain management combined with sedation can not only relieve the patient's discomfort and pain but also improve the success rate of intubation and avoid additional pain caused by repeated operations.
Pain management for bronchofiberscopy
A 2013 study found that remifentanil target-controlled infusion analgesia was reliable in ICU patients who required bronchoscopy with spontaneous breathing[26].
Kundra[27]evaluated the efficacy of upper airway anesthesia produced by nebulized lidocaine against a combined regional block(CRB)for awake fiberoptic nasotracheal intubation.The results showed that both nebulization and CRB produced satisfactory anesthesia of the upper airway,but CRB provided better patient comfort and hemodynamic stability[27].A randomized controlled study was performed to compare two methods of airway anesthesia,namely,ultrasonic nebulization of a local anesthetic and the performance of airway blocks.The results showed that upper airway blocks provided better quality anesthesia than lidocaine nebulization[28].
I realized that my waist-length hair was back in a ponytail, and that he wanted it to hang down. Perhaps he wanted to see it, like the horse s tail in front of us, free and swinging. Or perhaps I had worn it down in other classes with him and it wasn t the same today. For whatever reason, I knew he wanted me to free that ponytail, so I did. He looked at me, managed to touch his hands together a couple of times in what he used as clapping, and he smiled at me.
The above studies indicate that the analgesic effect of topical anesthesia combined with a nerve block is superior,but it may be difficult for some clinicians to achieve.On the basis of adequate topical anesthesia,combining intravenous analgesic sedative drugs may have a better effect,but this option needs to be confirmed by clinical research.
He thought he must have heard amiss, and rubbed his eyes, and said, Alas, wife, what are you saying? Husband, said she, if I can t order the sun and moon to rise, and have to look on and see the sun and moon rising, I can t bear it
Pain management of nasogastric tube intubation
Nasal tube intubation is a common operation in the ICU but a painful process for patients[29].Pain management for nasal tube intubation mainly involves topical anesthesia.
Most studies on the management of pain caused by arterial puncture and catheterization and PICCs focus on topical anesthesia.A review published in 2006 suggested that the use of lidocaine topical anesthesia before arterial puncture can significantly reduce pain and does not affect the success rate of puncture[12].In 2012,a randomized double-blind trial examined topical anesthesia induceda lidocaine/tetracaine patch in arterial puncture and showed that both the lidocaine/tetracaine patch and a subcutaneous injection of lidocaine effectively relieved pain during arterial puncture;however,the subcutaneous injection of lidocaine caused discomfort during the injection.In contrast,the lidocaine/tetracaine patch should be placed for 20 min before the operation,and the analgesic effect is better if given enough time[13].A study published in 2016 compared the analgesic effects of vapocoolant sprays(ethyl chloride and alkane mixtures)with lidocaine local anesthesia during radial artery cannulation.The results showed that vapocoolant sprays can replace local anesthesia with lidocaine to relieve pain and discomfort caused by arterial catheterization[14].A trial conducted in 2001 evaluated the effectiveness of two types of local anesthesia(buffered lidocaine and EMLA cream,which is a eutectic mixture of 2.5% lidocaine,2.5% prilocaine,an emulsifier,and a thickener)compared to no anesthesia.The results showed that buffered lidocaine was superior to EMLA cream or no anesthesia in reducing PICCrelated pain[15].
A randomized controlled trial by Singer and Konia[30]showed that using topical lidocaine and phenylephrine for the nose and tetracaine with benzocaine spray for the throat prior to nasogastric(NG)intubation resulted in significantly less pain and discomfort than using a nasal surgical lubricant alone.Widespread use of topical anesthetics and vasoconstrictors prior to NG intubation is recommended[30].Studies by Wolfe[31]have shown that atomized nasopharyngeal and oropharyngeal 4%lidocaine results in clinically and statistically significant reductions in pain during NG tube(NGT)placement.Ducharme and Matheson[32]compared atomized lidocaine,atomized cocaine,and lidocaine gel and found that 2% lidocaine gel appeared to provide the best option for a topical anesthetic during NGT insertion.A randomized controlled trial by Cullen[33]showed that nebulized lidocaine decreases the discomfort of NGT insertion and should be considered before passing an NGT.
Years have passed since then, and both our gardens and our friendship have continued to grow. That story has grown, too - to become one of our dearest bonds. I guess, true to form, I really will try to plant just about anything.
Both nebulized and topical local anesthetics(lidocaine,tetracaine,cocaine)can alleviate the pain of NG intubation.The combined application of both nebulized and topical local anesthetics may be a better option during NG intubation.
There is little research on analgesia after nasal jejunal intubation.In fact,management for nasal jejunal intubation may be patterned after pain management for NG tube intubation.
However, the good Fairy of the Beech-Woods did not want her to be starved, so she sent her an unlooked for relief in the shape of a beautiful white cow, which followed her back to the tiny house
Pain management of urethral catheterization
A randomized controlled trial in 2004 determined whether pretreatment of the urethra with topical lidocaine reduces the pain associated with urethral catheterization.The results showed that using a topical lidocaine gel can reduce the pain associated with male urethral catheterization in comparison with topical lubricants only[34].Another randomized controlled trial in 2007 compared the effects of a lidocaine gel and a water-based lubricating gel for female urethral catheterization.The results showed that compared with the water-based lubricating gel,the lidocaine gel substantially reduced the procedural pain caused by female urethral catheterization[35].
In addition,three studies compared whether the preuse of ice packs can alleviate the pain of chest tube removal.Integration of the three studies in a meta-analysis showed that the preuse of ice packs can alleviate the pain of patients with chest tubes.The pain score was reduced after removal of the chest tube,SMD=0.30,[95% confidence interval(CI):0.01-0.59,= 0.04,= 0%][43-45].
All of the above studies have shown that topical anesthesia with a lidocaine gel can effectively reduce the pain experienced during urethral catheterization.The management of pain caused by natural cavity noninvasive catheterization is shown in Table 3.
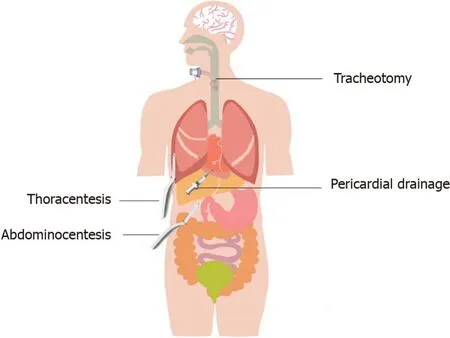
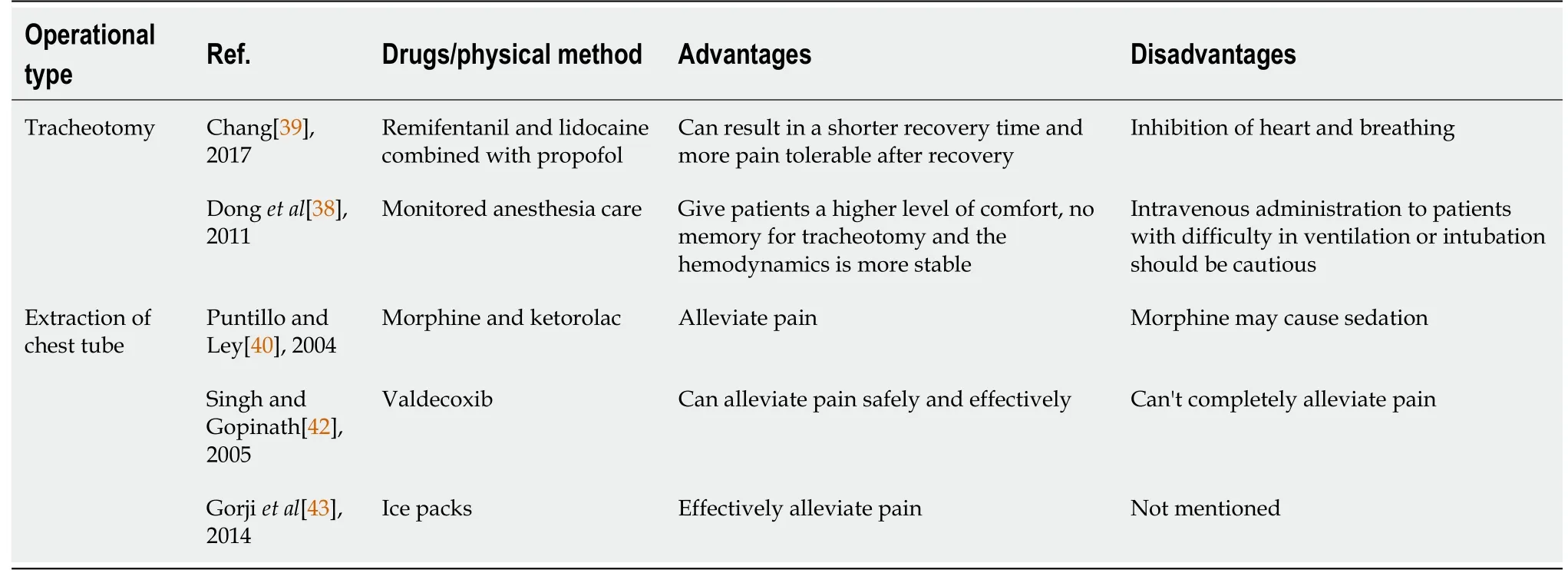
MANAGEMENT OF PAlN CAUSED BY NATURAL CAVlTY PERCUTANEOUS CATHETERlZATlON AND EXTUBATlON
Natural cavity percutaneous catheterization is common in the ICU(Figure 3).Tracheotomy can quickly establish a respiratory passage and save patients' lives;thoracentesis,thoracic closed drainage,pericardial drainage,and abdominocentesis can drain effusions or gas to relieve symptoms and to diagnose and treat diseases.Since these operations require puncture through the skin and muscle layers,pain management is necessary.
Pain management of tracheotomy
A 2014 study by Samantaray and Rao[16]evaluated the efficacy of fentanyl combined with local infiltration anesthesia with lidocaine for CVCs.The results showed that fentanyl is effective in relieving pain and can be safely used in conscious patients.The same team compared the effects of dexmedetomidine,fentanyl,and placebo during CVC placement in a trial conducted in 2016.The study concluded that both dexmedetomidine and fentanyl achieved good analgesia.Dexmedetomidine is superior to fentanyl and placebo in providing comfort to patients but is associated with excessive sedation and cardiovascular adverse events[17].The latest study conducted in 2019 compared the target-controlled infusion of remifentanil plus local lidocaine infiltration and placebo plus local lidocaine infiltration in conscious patients.Remifentanil is effective in reducing the pain associated with local lidocaine infiltration during CVC placement[18].
A 2011 trial compared local anesthesia(2% lidocaine tracheal mucosal-surface anesthesia and local-infiltration anesthesia)and monitored anesthesia(midazolam,propofol and fentanyl given intravenously after surface and local anesthesia)during tracheotomy.Monitored anesthesia gave patients a higher level of comfort,no memory of the tracheotomy and more stable hemodynamics[38].A recent study evaluated the pain management and side effects of remifentanil in percutaneous dilatational tracheostomy.The results showed that based on propofol general anesthesia,combined treatment with remifentanil and lidocaine for local anesthesia can result in a shorter recovery time and more tolerable pain after recovery[39].
Tracheotomy pain management has mostly focused on intravenous analgesia(fentanyl,remifentanil),sedative drugs(propofol,midazolam)and combination treatment with local infiltration anesthesia(lidocaine),which can provide good pain management and sedative effects.According to the patient's circulatory state and the original pain management sedation plan,the pain management sedation combination and the local infiltration anesthesia method can be selected.
Then Little Two-eyes came out from under the cask quite happily, and the knight was astonished at her great beauty, and said, Little Two-eyes, I am sure you can break me off a twig from the tree
Pain management for the extraction of a chest tube
A 2004 study compared morphine and ketorolac in cardiac surgery patients undergoing chest tube removal.The findings confirmed that if used correctly,either an opioid(morphine)or an NSAID(ketorolac)can substantially reduce pain during chesttube removal without causing adverse sedative effects[40].However,a review published in 2005 suggested that morphine alone does not provide satisfactory pain management for chest tube removal pain.NSAIDs,local anesthetics and inhalation agents may play a role in providing more effective analgesia[41].
A prospective,randomized,double-blind,placebo-controlled study conducted in 2005 evaluated the efficacy of topical valdecoxib as an analgesic during chest tube removal in postcardiac surgical patients.The results showed that compared with liquid paraffin,valdecoxib is a safe and effective topical analgesic[42].
The sky was blue, and a fresh breeze played on their faces; but how melancholy8 everything looked all around! Her father s castle lay in ruins, the town and the villages were, so far as could be seen, destroyed by fire, the fields far and wide laid to waste, and no human being was visible
There are many pain management methods,such as intravenous opioid analgesics,NSAIDs and cold compresses,for the extraction of chest tubes.There are few studies on local infiltration anesthesia,but it may be a better pain management method for the extraction of chest tubes because local infiltration anesthesia not only reduces pain during extubation but also reduces pain after extubation.The effect of local infiltration anesthesia in the extraction of chest tubes needs to be confirmed by clinical studies.
At present,pain caused by arterial puncture and catheterization,deep venous catheterization,and PICCs in the ICU is usually managed by local infiltration anesthesia.However,local infiltration anesthesia has the following limitations:(1)Local infiltration anesthesia itself can cause pain;(2)The effect of partial local infiltration anesthesia is not perfect;(3)After local infiltration,superficial arteriovenous structures may be difficult to identify,increasing the difficulty of puncture;and(4)Improper operation of local infiltration anesthesia may cause local anesthetic poisoning.Therefore,some clinical studies have attempted to apply more pain management methods to alleviate the pain caused by the establishment of vascular access.
MANAGEMENT OF PAlN CAUSED BY OTHER PROCEDURES
Some nursing care in the ICU can also cause discomfort to the patient,and appropriate pain management can reduce the incidence of pain and adverse events.
Pain management of turning
Turning is part of routine nursing care that is beneficial to sputum discharge and can even prevent hemorrhoids.However,due to the patient's own disease and the presence of various tubes,the patient may suffer from pulling and friction pain during turning.Even if the movement is slow and gentle,it will cause discomfort and pain to the patient.
In a randomized controlled trial conducted by Robleda[46],patients who underwent mechanical ventilation in the ICU were randomized to a fentanyl group(39 patients)and a placebo group(36 patients).Fentanyl or placebo was administered before turning.The incidence of pain in the fentanyl group was lower than that in the control group,and the incidence of adverse events was not statistically significant in the fentanyl group[46].
A prospective intervention study by de Jong[47]found that planned analgesia treatment(analgesic drugs combined with music)before turning can reduce the incidence of severe pain from 16% to 6%(odds ratio = 0.33,95%CI:0.11-0.98,= 0.04)and the incidence of serious adverse events from 37% to 17%.
Now Christian was a merry fellow who liked good company; he could both drink and sing, and talk and boast as well, when he got a little drop in his head
Morning came, and the king got up, pale and sulky, and, after learning from the hermit which path to take, was soon mounted and found his way home without much difficulty
At present,no more attention is being paid to pain management during patient turning.Because the pain caused by turning is mostly systemic,general anesthesia may be a good choice.Remifentanil can be chosen because it has a quick effect and a short half-life;moreover,its analgesic effect and side effects are dose-dependent,so it is suitable for turning.The management of pain caused by other procedures is shown in Table 5.

Since some ICU patients are already in a state of analgesia and sedation during the above operations,the combination of local anesthesia(surface anesthesia or local infiltration anesthesia)on the basis of deepening their analgesia and sedation may be a more effective pain management method for procedural pain.However,for patients who are not under analgesic sedation,the pain management methods mentioned above can be referred to.
Eveqbody worked to keep the garden growing. All summer long, the family ate food from the garden and enjoyed the beautiful flowers.Grandma put up strawberry jam, tomatoes, beans, peppers, pears and peaches in canning jam. They were good to eat through the long winter.
Critical care medicine aims to provide the most comprehensive and effective life support for patients with multiple organ dysfunction and severe nonterminal diseases to save their lives,improve their prognosis to the greatest extent and increase their quality of life.Contemporary medicine focuses on human care.Pain management in the ICU can eliminate or alleviate pain and discomfort,reduce adverse stimuli and excessive sympathetic nervous system excitement,facilitate and improve sleep,induce procedural amnesia,reduce memory in the ICU,alleviate or reduce anxiety,incite or even paralyze,prevent unconscious movements,reduce the metabolic rate and decrease oxygen consumption to ensure organ metabolism.
CONCLUSlON
Pain management is a process of continuous quality improvement that requires multidisciplinary team cooperation,pain-related training of all relevant personnel,effective relief of all kinds of pain,and improvement of patients' quality of life.In clinical work,which involves complex and diverse patients,we should pay attentionto the following points for procedural pain:(1)Consider not only the patient's persistent pain but also his or her procedural pain;(2)Conduct multimodal pain management;(3)Provide combined sedation on the basis of pain management;and(4)Perform individualized pain management.Until now,the pain management of procedural pain in the ICU has not attracted extensive attention.There are few studies and there is no clear standard for the application of drugs;thus,there is no adequate guidance for clinicians to use exact treatment methods to reduce patients' pain and improve their prognosis.Moreover,for some special procedures,such as ECMO and CRRT,we should provide individualized pain management based on pharmacokinetics and pharmacodynamics.Therefore,we expect additional studies to solve the existing problems of procedural pain management in the ICU.
 World Journal of Clinical Cases2022年5期
World Journal of Clinical Cases2022年5期
- World Journal of Clinical Cases的其它文章
- Subclavian artery stenting via ilateral radial artery access:Four case reports
- Neurothekeoma located in the hallux and axilla:Two case reports
- Diffuse invasive signet ring cell carcinoma in total colorectum caused by ulcerative colitis:A case report and review of literature
- Tacrolimus treatment for relapsing-remitting chronic inflammatory demyelinating polyradiculoneuropathy:Two case reports
- Aseptic abscess in the abdominal wall accompanied by monoclonal gammopathy simulating the local recurrence of rectal cancer:A case report
- Unusual magnetic resonance imaging findings of brain and leptomeningeal metastasis in lung adenocarcinoma:A case report