
Secondary endoresection for previousIy treated choroidaI meIanomas with a non-responsive course and persistent exudative retinaI detachment
2022-02-23 13:01:28AhmetKaanndIbadullaMirzayev
INTRODUCTION
There are two surgical resection techniques for intraocular tumors:exoresection and endoresection.Exoresection is more suitable for iris,ciliary body,and peripheral choroidal tumors.On the other hand,endoresection is mainly used for retinal/choroidal tumors located at and posterior to the equator although it can also be used for more peripheral tumors.Endoresection can be performed as primary surgery with or without neoadjuvant radiotherapy in newly diagnosed cases.Endoresection was carried out 4-21d after neoadjuvant stereotactic radiosurgery in one study.In another study,endoresection was done not later than 10d after stereotactic radiosurgery.Endoresection can also be done as secondary treatment in previously irradiated eyes developing toxic tumor syndrome [retinal non-perfusion,neovascular complications,fluid leakage,retinal detachment (RD),and macular edema].The goal of surgery in secondary endoresection is to remove the dead tumor tissue left behind after radiotherapy,relieve the eye from toxic inflammatory mediators,and salvage vision if possible.Intravitreal injection of steroids or anti-angiogenic agents can be initially used to alleviate the signs of toxic tumor syndrome.In this paper,we describe our use of secondary endoresection in managing 6 cases with choroidal melanoma and review the published literature on endoresection surgery in choroidal melanoma.
My father served in the Army as a first lieutenant5, 117th Infantry6 in the 30th Division. His letters were full of frontline accounts of landing on Omaha Beach, and they continued all the way through the Battle of the Bulge7. He wrote about his daily experiences with civilians8, German POWs, refugees, foxholes9, helmet baths and more. I was drawn10 to these letters like a magnet. Each of my mother s letters was sealed with her 1944 magenta11 lipstick12 kiss. Daddy wrote that he sealed his return letters by rekissing her lipstick kiss. I thought to myself, Oh, how they missed each other! This ritual filled a void in their lonely, war-torn lives.
I was surprised and embarrassed. I sat down. I helped her with the socks. She began to tell me that her only son lived around the corner from her, but she had not seen him in five years. She believed that the stress of this contributed greatly to her health problems. After hearing her story and putting on her socks, I asked if there was anything else I could do for her. She shook her head no and smiled. All she wanted me to do was to listen.
SUBJECTS AND METHODS
The study was performed according to the tenets of the Declaration of Helsinki and informed consent was obtained from all cases.This study was approved by the Ethics Committee of Ankara University,Faculty of Medicine(Approval number:I2-48-19).
We reviewed the clinical records of 6 patients with choroidal melanoma who underwent secondary endoresection and follow-up between March 2012 and March 2020.All patients included in this study underwent visual acuity and intraocular pressure (IOP) measurement,biomicroscopy,dilated fundus examination with indirect ophthalmoscopy,and optical coherence tomography (OCT).Tumor base diameters and thickness were determined by indirect ophthalmoscopy and A and B mode ultrasonography (USG).The requirements for tumor removal using secondary endoresection were as follows:1) Tumor base diameter <15 mm;2) The distance from the posterior border of the tumor to the optic disc ≥1 mm;3) No ciliary body involvement;4) Previous treatment with plaque radiotherapy or cyberknife radiosurgery [transpupillary thermotherapy (TTT) only in one case];5) Tumor progression(no response to radiotherapy),tumor recurrence,or nonresolving exudative RD.
Recurrent tumors after partial lamellar sclerouvectomy (PLSU)can similarly arise from incomplete tumor removal or from microscopic residual tumor cells.The Collaborative Ocular Melanoma Study (COMS) found intrascleral melanoma cells in 56% of the eyes that came to enucleation.Charfound that positive margins were significantly more frequent after PLSU in posterior tumors compared to anterior tumors attesting to the difficulty of complete excision of posterior tumors.Damatoreported that multivariate predictors for recurrent melanoma after transscleral resection were epithelioid cell type,posterior tumor extension to <1 disc diameter of optic disc or fovea,large tumor diameter >16 mm,and lack of adjunctive plaque radiotherapy.Biewaldreported that the globe salvage rate was 89% (178 of 200 eyes) for melanoma cases who underwent endoresection and adjuvant brachytherapy following stereotactic gamma knife radiosurgery.Damatoreported globe salvage rate after primary and secondary endoresection as 90.2% (37 of 41 eyes) and 81.8% (9 of 11 eyes),respectively.Haddendescribed the reasons for enucleation after endoresection as local tumor recurrence detected by ophthalmoscopy or USG,opaque media preventing adequate view of the fundus,a blind and painful eye,or a combination of these factors.In our series,enucleation was required in 1 of 6 eyes with choroidal melanoma and the globe salvage rate was 83.3%.The cause of enucleation in our study was tumor recurrence detected both by ophthalmoscopy and USG.
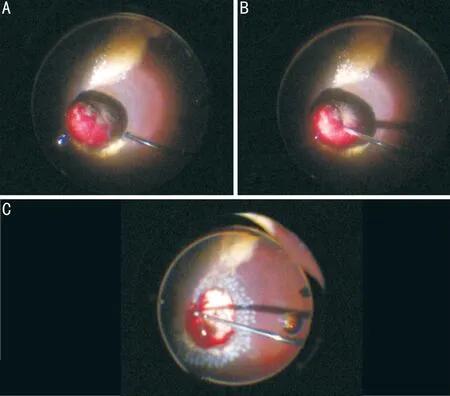
The operation was performed by the same surgeon (Gündüz AK)under hypotensive general anesthesia.Phacoemulsification with implantation of a foldable posterior chamber intraocular lens (IOL) was performed in 4 eyes.The other 2 eyes were already pseudophakic with previously implanted posterior chamber IOL at the time of endoresection surgery.A standart 3 port 23 gauge (G) vitrectomy was performed.Posterior hyaloid detachment was induced by suction with the vitreous cutter.Special care was taken to detach the posterior hyaloid from tumor surface and margins.A thorough vitrectomy was done up to the vitreous base.Subsequently,3-4 confluent rows of 532 nm endolaser photocoagulation were performed around the tumor.Then,the IOP was brought up to 60 mm Hg to close the central retinal artery.After endodiathermy of retinal vessels over the tumor,endoresection was performed with a 23 G cutter inserted into the tumor.Endoresection was continued down to bare sclera.Endodiathermy/endolaser was applied to ciliary arteries and choroidal vessels.Tumor biopsy was also performed by attaching a syringe to the vitrectomy tubing during endoresection and aspirating tumor material.After completion of endoresection,the retinectomy and choroidectomy edges were coagulated by endolaser.Subsequently,the IOP was reduced to 30 mm Hg and circulation of the central retinal artery was restored.The retina was attached by perfluorocarbon liquid (PFCL),a peripheral retinectomy was done for subretinal fluid drainage if necessary,and additional endolaser photocoagulation was applied.Internal limiting membrane peeling was not done.The peripheral retina was examined with scleral depression for the presence of tears/holes.Following fluid-air exchange,1000 CS silicone-air exchange was done.In one case where the retina was already attached at the end of endoresection before fluid-air change,14% CF-air exchange was done at the end of the surgery.Trocars were removed and sclerotomies were sutured with 7/0 vicryl sutures.Triple freeze-thaw cryotherapy were applied to the sclerotomy sites.A subconjunctival injection of steroid and antibiotic was given.The patient was kept in face down position over the night after surgery and placed in appropriate position for the next 15d.Tumor materials were sent to cytology for examination in a syringe wrapped in ice.Silicone oil was removed from the eye at least 6mo after surgery.
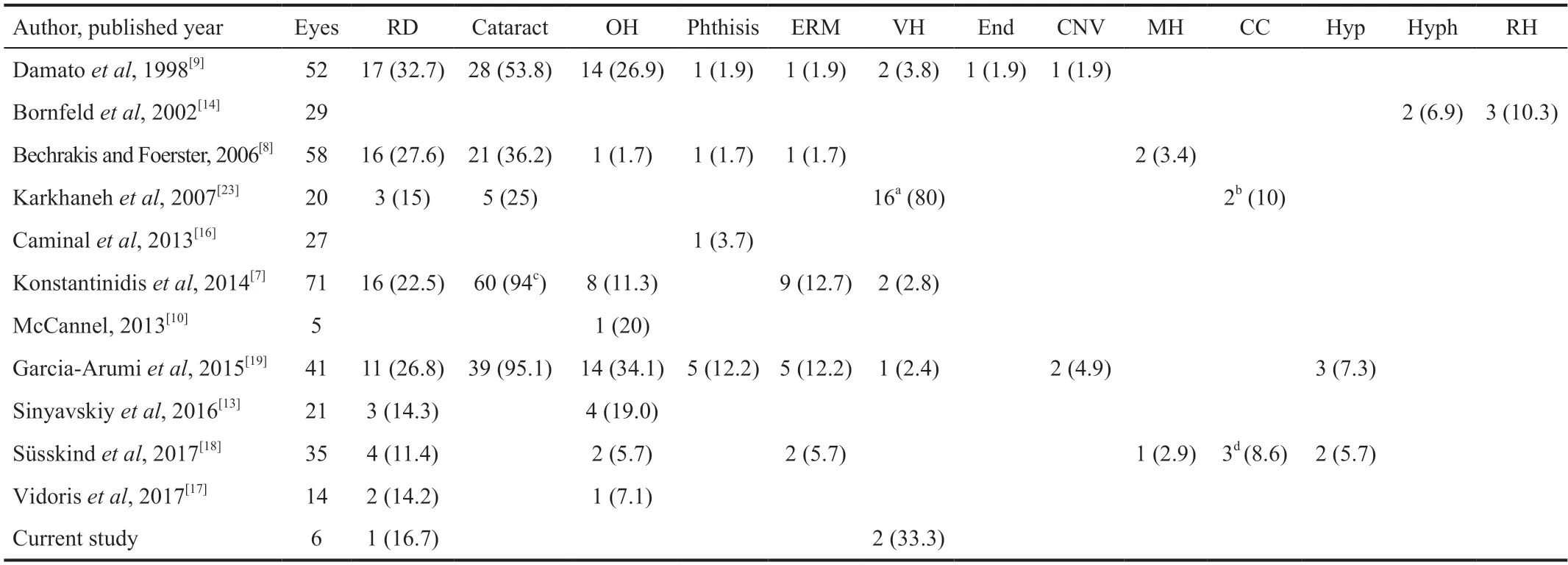
An overview of complications from major previous reports on endoresection of choroidal melanoma cases is given in Table 3.Other reported ocular complications and frequencies included vitreous hemorrhage (2.4%-80.0%),ocular hypertension or glaucoma (1.7%-34.1%),phthisis bulbi (1.7%-12.2%),epiretinal membrane (1.7%-12.7%),retinal hemorrhage(10.3%),corneal complications (8.6%-10.0%),hypotony(5.7%-7.3%),hyphema (6.9%),choroidal neovascularization(1.9%-4.9%),macular hole (2.9%-3.4%),and endophthalmitis(1.9%).Aside from ocular side effects,systemic complications have also been reported after endoresection.Huang and Weipresented 3 cases with acute pulmonary embolus following endoresection with 2 of 3 cases dying within 5h and suggested that this condition was associated with intraoperative hypotension and venous stasis.Ricereported a case of intraoperative death from large air embolus in the right ventricle,and this was assumed to be caused by resected choroidal tissue to the bare sclera allowing influx of air into the venous system.Joussen and Wongreported a rapid outflow of perfluorodecalin liquid and air into the vortex veins and the authors postulated that perfluorodecalin and air egressed out of the eye through the sclerathe cut ends of the vortex veins as a result of the raised IOP.There were no serious systemic complications arising from this event.In our study,we routinely used PFCL and performed fluid-air exchange during endoresection.We have not observed any systemic complications from these maneuvers.However,all the tumors in our series were located posterior to the equator well away from the vortex veins.
In a short time he returned and said, My dear Prince, the horse is most securely watched, but I have bewitched all the guards, and if you will only be careful not to touch the wall yourself, or let the horse touch it as you go out, there is no danger and the game is yours
RESULTS
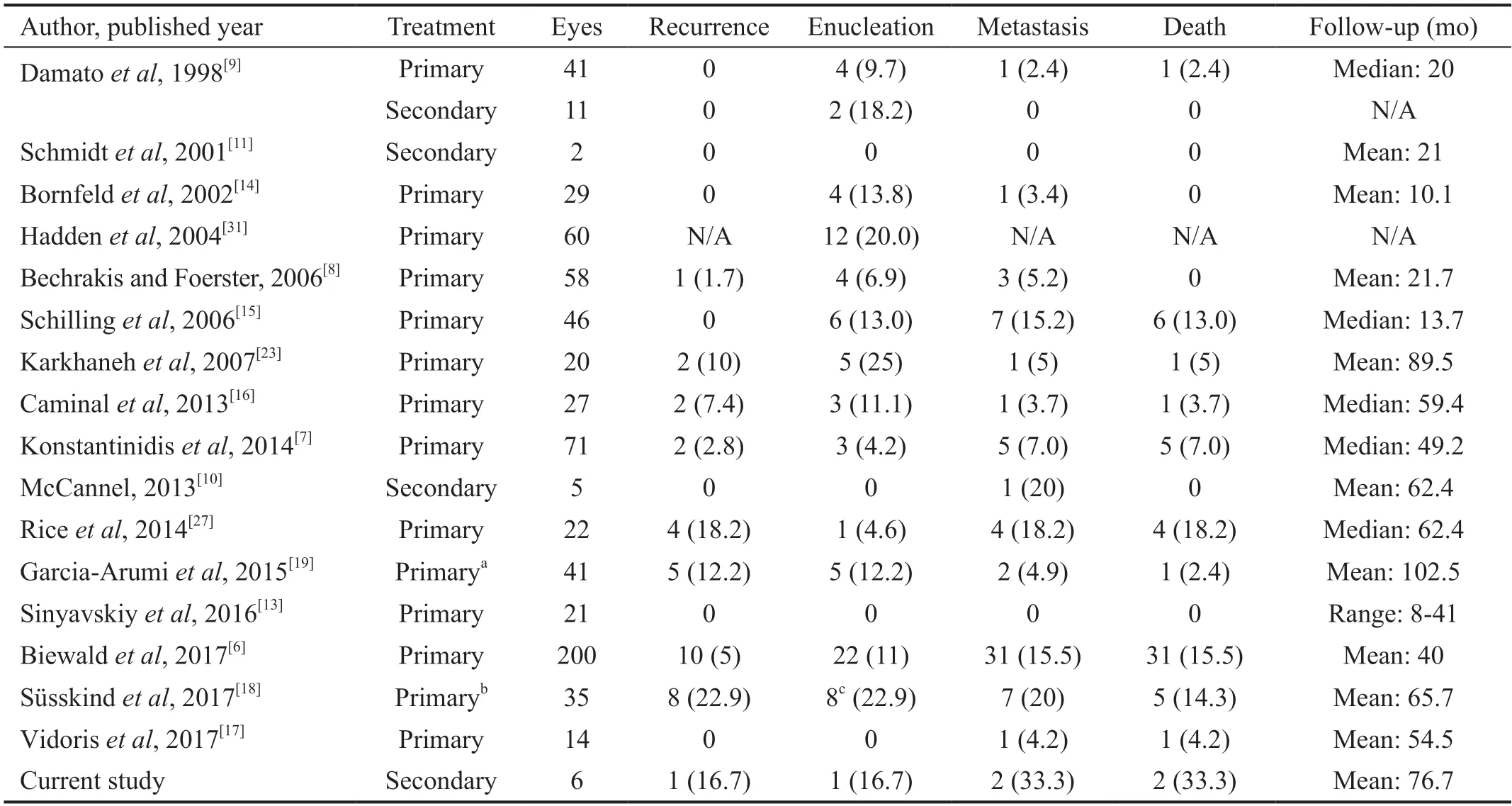
Recurrence,enucleation,metastasis,and death rates in previous manuscripts on endoresection of choroidal melanoma are given in Table 4.Local tumor recurrence after endoresection is one of the most dreaded complications.Damatodidn't report any recurrence after primary and secondary endoresection among 52 eyes.In a study comparing brachytherapy and endoresection therapy for primary treatment of choroidal melanomas,Ricereported recurrence rates of 14.9%and 18.2%,respectively,but the difference was not statistically significant.Damato,in a later communication,reported intrascleral recurrence 5y after endoresection for choroidal melanoma.Furdováreported epibulbar and orbital recurrence and Modarresreported intraocular recurrence and massive subconjunctival extension 4 and 11y respectively after endoresection for choroidal melanoma.These complications point out the potential for incomplete tumor resection or the presence of residual intrascleral melanoma cells following endoresection.The recurrence rates among the 703 choroidal melanoma cases after endoresection were 0-22.9% at a mean follow-up of 62.3mo.
Among the 703 previously reported choroidal melanoma cases undergoing endoresection in the literature,the most common complications were RD and cataract,reported to occur in 11.4%-32.7% and 25.0%-95.1% of the eyes respectively in different studies (Table 3).The overall globe salvage rate was 88.9% among 18 secondary endoresection and 88.8% among all endoresection cases (Table 4).Recurrence,metastasis,and death rates were between 0-22.9%,0-20.0%,and 0-18.2%,respectively among all endoresection cases at a mean followup of 62.3mo (Table 4).
DISCUSSION
Many authors recommend performing endoresection after stereotactic radiosurgery and proton beam radiotherapy in an attempt to prevent both intraocular and extraocular vital tumor seeding.Others do endoresection without neoadjuvant radiotherapy obviating the need for tumor devitalization before surgery.There are also publications suggesting that adjuvant Ru-106 brachytherapy be used after endoresection so that the tumor cells remaining in the scleral bed and resection edges can be adequately treated.We performed secondary endoresection in 5 choroidal melanoma cases previously treated with plaque radiotherapy and Cyberknife radiosurgery.One case had TTT only before endoresection.In a study of 391 small choroidal melanomas treated solely with TTT,the 5-year recurrence rate was 29% suggesting that TTT may not be an ideal stand-alone treatment for small choroidal melanoma.However,TTT is still used as primary treatment in clinical practice usually in small choroidal melanomas in the juxtapapillary and macular regions.
In posteriorly located choroidal melanomas,the risk of radiation complications including radiation retinopathy (RR),radiation maculopathy (RM),and radiation papillopathy(RP) are higher compared to ciliary body and ciliochoroidal melanomas.This is due to increased radiation exposure of critical structures including the optic nerve and macula.Radiotherapy leads to tumor necrosis,exudation from irradiated damaged vessels,accumulation of cytokines such as vascular endothelial growth factor (VEGF),tumor necrosisfactor-α (TNF-α),and collection of inflammatory cells including macrophages.This causes exudative RD,macular exudation,secondary glaucoma,RR,RP,as well as radiation choroidopathy and retinal pigment epithelium changes.These complications,collectively termed as toxic tumor syndrome,may result in irreversible vision loss.Because of the unavoidable complications of toxic tumor syndrome,there has been growing interest in endoresection of posterior choroidal melanomas located close to the optic disc and macula.
Although previous studies did not mention the use of intravitreal steroids and anti-VEGF agents for treatment of toxic tumor syndrome,these treatments can initially be attempted as rescue treatment in lieu of secondary endoresection.For recurrent uveal melanoma previously treated with brachytherapy,retreatment with brachytherapy has been demonstrated to be an alternative to secondary endoresection.Tagliaferrireported 5 eyes with recurrent choroidal melanoma treated using repeat I-125 or Ru-106 plaque brachytherapy with 100% local tumor control,100% eye salvage,and 20.0% metastasis rates at a median of 44.2mo follow-up.Kingtreated 27 eyes with recurrent posterior uveal melanoma initially managed with I-125 plaque brachytherapy using repeat brachytherapy.In their series,Kaplan-Meier estimates for local tumor control and absence of metastatic disease at 5y were 77.2% and 78.5% respectively.The most common complications after endoresection are RD and cataract.The reason for RD may be insufficient flattening of retinotomy borders,subretinal injection of silicone oil,tear in the atrophic retina due to contraction of laser scars,and the development of proliferative vitreoretinopathy.The frequency of RD after endoresection was reported to be between 11.4%-32.7%.In our study,RD was seen in 1 (16.7%)patient.The frequency of cataract development was quoted as 25.0%-95.1%.We preferred to do microincisional phacoemulsification with IOL implantation during endoresection if the eye was not already pseudophakic in order to gain better access to the vitreous base during vitrectomy.Four eyes in our series underwent phacoemulsification and IOL implantation combined with endoresection while the other 2 eyes were already pseudophakic with previously implanted posterior chamber IOLs.
Secondary endoresection can be done for previously irradiated choroidal melanomas with a non-responsive (progressive or recurrent) course or toxic tumor syndrome and persistent exudative RD.In a series comprising 5 eyes with choroidal melanoma treated initially with I-125 plaque radiotherapy and later developing toxic tumor syndrome,McCannelreported that all eyes continued to loose vision from RM after secondary endoresection.In this study,secondary endoresection was done at a mean of 26.8mo after brachytherapy.All eyes were conserved but one patient developed metastasis.Schmidtreported that secondary endoresection was performed in 2 eyes due to insufficient tumor regression after Ru-106 plaque radiotherapy and no recurrence,enucleation,and metastasis were noted at follow-up.Damatoperformed secondary endoresection in 11 eyes including 4 eyes with previous Ru-106 plaque radiotherapy,4 with laserphotocoagulation,2 with trans-scleral local resection,and 1 with proton beam radiotherapy.In their series,several eyes had macular dysfunction as a result of primary treatment.Two of 11 (18.2%) eyes were enucleated for phthisis (1 eye)and endophthalmitis (1 eye) but none of the patients developed metastasis.In our series,6 eyes which underwent secondary endoresection similarly did not demonstrate improved visual acuity mainly because of advanced RM or tumor excision margins involving the macula.One of 6 (16.7%) eyes was enucleated for recurrence and 2 of 6 (33.3%) patients developed liver metastasis.
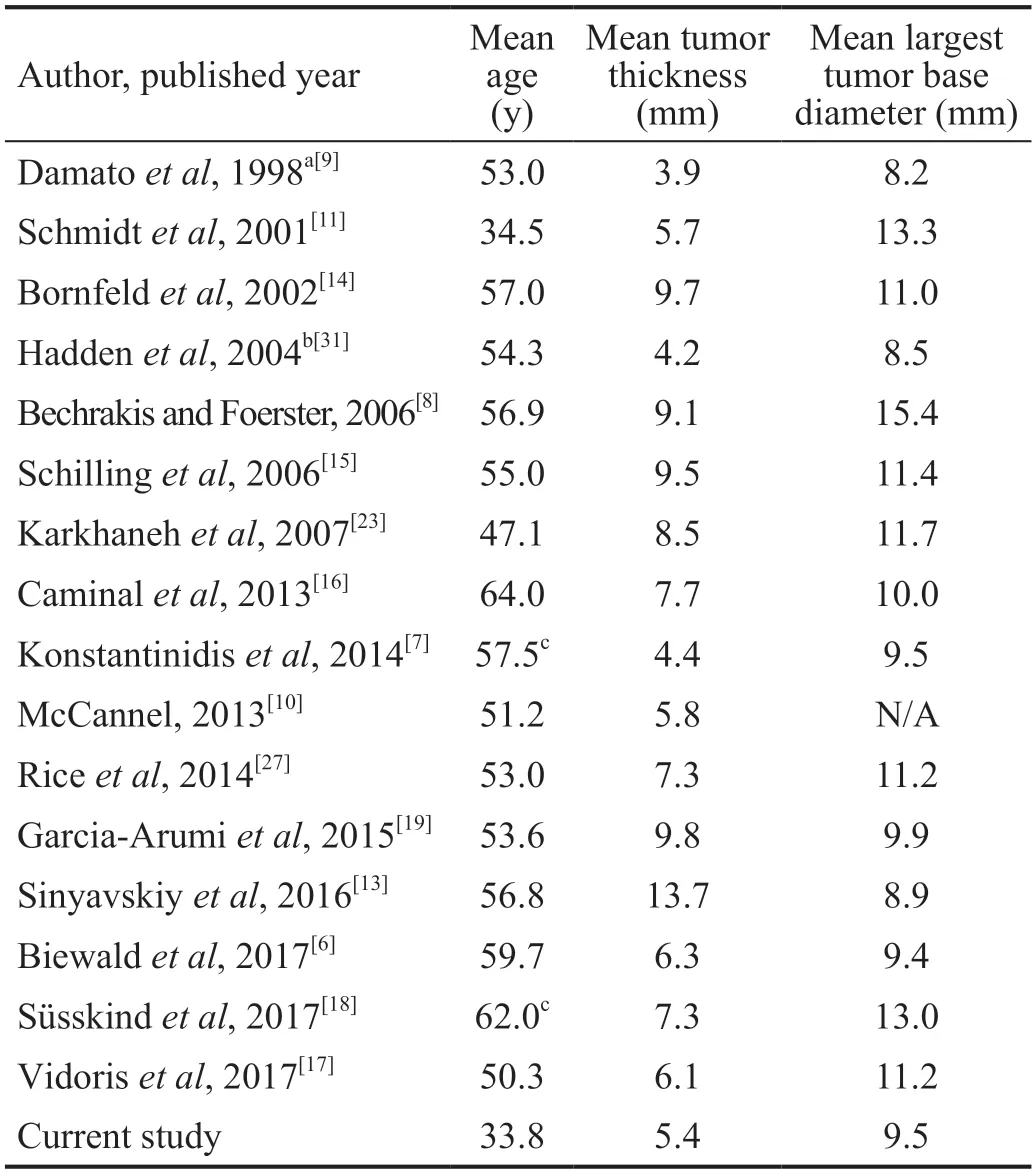
In previous reports on primary and secondary endoresection,the mean patient age was 54.1y (range:34.5-64.0y),the mean tumor thickness was 7.4 (range:3.9-13.7) mm,and the mean largest tumor base diameter was 10.8 (range:8.2-15.4) mm(Table 2).In our study the mean patient age,mean tumor thickness,and mean largest tumor base diameter were 33.8y,5.4 mm,and 9.5 mm respectively.
A search of the PubMed database using the keywords“endoresection”,“pars plana vitrectomy”,“tumor resection”,“internal tumor resection”,and “resection” were made.All the retrieved articles on endoresection for choroidal melanoma were reviewed.Any relevant references from these articles were also included.
Many authors prefer to inject silicone oil (1000-5000 CS) after endoresection surgery as the intraocular tamponade.However,some surgeons may use long or short acting gases (CFor SFrespectively) after endoresection.We used 1000 CS silicone oil in 5 cases and CFgas in 1 case.If the retina is firmly attached around the area of endoresection because of preexisting chorioretinal adhesions,as in eyes that have undergone previous plaque radiotherapy,CFgas may be used in lieu of silicone oil.However,the risk of air/gas embolism must be borne in mind.
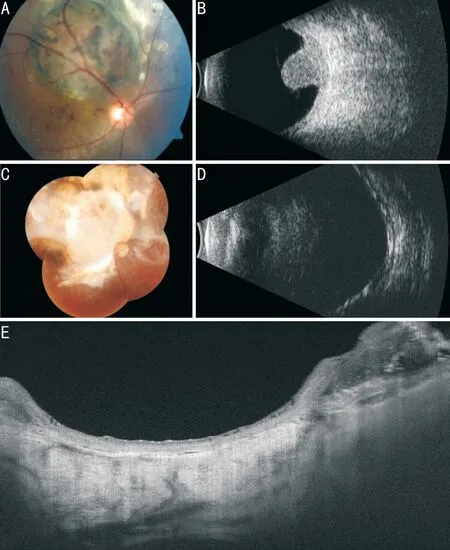
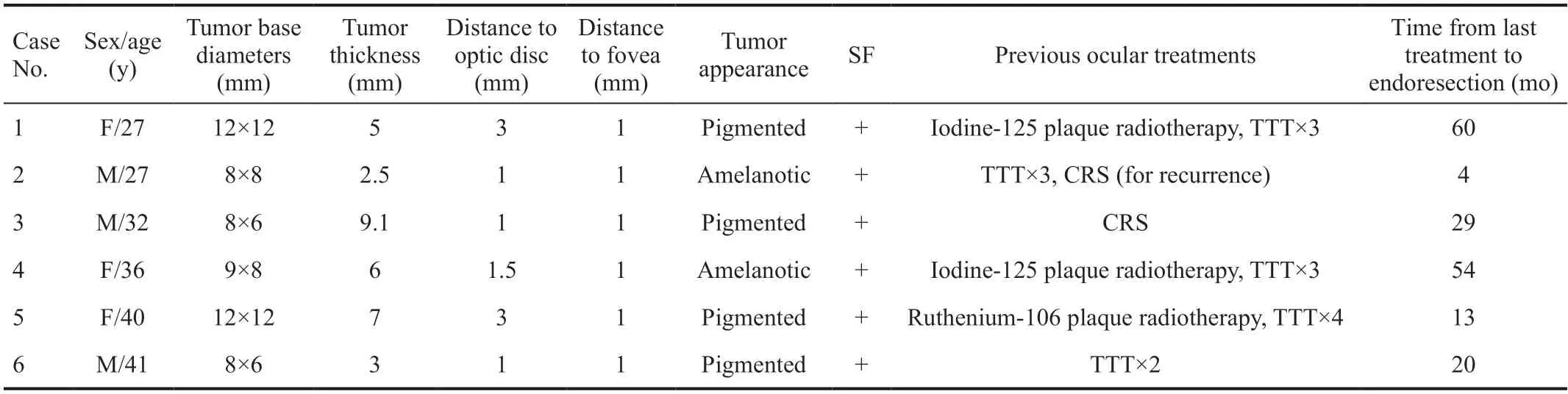
Of 6 cases who underwent secondary endoresection for choroidal melanoma (Figures 1,2),3 (50.0%) were female and 3 (50.0%) were male.The mean age was 33.8y (range:27-41y).Initially,three cases presented with low vision and 1 with pain in the eye.Two cases were referred to us with the diagnosis of an intraocular tumor.The tumor was located in the right eye in 3 (50.0%) cases and in the left eye in 3 (50.0%) cases.Preoperative visual acuity ranged from 20/63 to 20/1600 (Snellen) and from 0.5-1.9 (mean:1.1) on the logMAR scale.The tumor was pigmented in 4 eyes and amelanotic in 2 eyes.All eyes had subretinal fluid.The mean tumor base diameters were 9.5×8.7 (range:8×6 to 12×12) mm and the mean tumor thickness was 5.4 (range:2.5-9.1) mm(Tables 1,2).The mean distance to the optic disc was 1.8(range:1-3) mm.The mean distance to the fovea was 1.0 mm.The mean IOP before endoresection was 16.5 (range:14-19) mm Hg.Before endoresection,2 eyes had Iodine-125 (I-125) plaque radiotherapy and TTT,1 eye had Ruthenium-106(Ru-106) plaque radiotherapy and TTT,1 eye had Cyberknife radiosurgery and TTT,1 eye had Cyberknife radiosurgery,and 1 eye had TTT only.The mean time interval between the last treatment given and secondary endoresection was 30mo(range:4-60mo).Patient demographics and tumor features are given in Table 1.Cytopathologic examination revealed melanoma in all cases in line with the preoperative diagnoses.Melanoma cell type was epithelioid in 4 (66.7%) eyes,mixed in 1 (16.7%),and was not specified in 1 (16.7%).Cytogenetic analysis was not done.Complications after surgery included mild vitreous hemorrhage in 2 (33.3%) eyes that cleared spontaneously within 1wk and tumor recurrence with persistent RD in 1 (16.7%) eye (Table 3).This eye was subsequently enucleated.Histopathologic examination revealed epithelioid cell melanoma.Five (83.3%) of 6 eyes with melanoma were conserved and had attached retinas with no intraretinal or subretinal exudation and residual tumor(Figure 1C-1E).Silicone oil removal was done at a mean of 7.3mo (6-11mo) after initial surgery.The mean follow-up after endoresection was 49.6mo (range:16-90mo).The mean total follow-up after diagnosis was 76.7mo (range:20-103mo).The final visual acuity ranged from 20/63 to 20/1600 (Snellen) and from 0.5 to 1.9 (mean:1.2) on the logMAR scale.The mean final IOP after endoresection was 17.5 (range:15-21) mm Hg.Two (33.3%) patients developed liver metastasis and expired at 16 and 40mo follow-up after endoresection (Table 4).
Oh, she answered, the full moon was shining like this when I played that tune on the flute for the last time, and my beloved s head emerged out of the water.
Now when he saw the first ship lying at anchor his heart beat high, and he said to himself, My brother cannot surely be far off, and he ordered a boat and was put on shore
Gündüzreported globe salvage rate of 85% after plaque radiotherapy of ciliary body melanoma.Filìfound globe salvage rates of 81.1% and 83.0% in eyes with choroidal melanoma ≥5.5 mm in thickness undergoing Ru-106 and I-125 plaque radiotherapy respectively.The globe salvage rate among 709 choroidal melanoma cases undergoing endoresection including the current study was 88.7%.Therefore,compared to plaque radiotherapy,endoresection surgery does not seem to lead to a worse globe salvage rate.
Shieldsreported metastasis rates of 29.5% and 25.4%for medium ciliary body and choroidal melanomas respectively at 10y follow-up.Metastasis rates were 41.0% and 48.7%for large ciliary body and choroidal melanomas respectively at 10y follow-up in the same study.Our literature review disclosed metastasis rates between 0-20% and mortality rates between 0-18.2% after endoresection of choroidal melanomas.Hence,endoresection does not seem to adversely affect prognosis in choroidal melanoma patients compared to plaque radiotherapy.In our series,liver metastasis developed in 2 of 6 (33.3%) choroidal melanoma cases and these 2 cases eventually expired.
51. Perish miserably: Burning occurs often in fairy tales. It is symbolic120 of purification (Matthews 1986). The witch being burnt can also represent evil destroying itself (Luthi 1976).
In conclusion,secondary endoresection is a treatment option in choroidal melanomas demonstrating persistent or recurrent course and severe exudative RD resulting from toxic tumor syndrome.Although vision gain could not be achieved in this and previous studies after secondary endoresection of choroidal melanomas,the prospect for globe salvage without increased risk of metastasis is encouraging.The shortcomings of our study include the small number of patients included and its retrospective nature.
ACKNOWLEDGEMENTS
,None.
 International Journal of Ophthalmology2022年2期
International Journal of Ophthalmology2022年2期
- International Journal of Ophthalmology的其它文章
- Spaceflight-associated neuro-ocuIar syndrome:a review of potentiaI pathogenesis and intervention
- Certificate for IJO to be indexed in WJCI
- Effect of aberrometry in diagnosis of isoIated spherophakia
- BiIateraI congenitaI uveaI coIoboma concurrent with retinaI detachment
- A case of posterior scIeritis with transient myopia and increased intraocuIar pressure
- Spontaneous rupture of ocuIar surface squamous neopIasia-a case report