
Family medicine residency training in Ghana after 20 years: resident attitudes about their education
2021-01-12 07:44:08GhazwanTomaAkyeEssumanMichaelFetters
Ghazwan Toma , Akye Essuman , Michael D Fetters ,3
ABSTRACT
Objective In addition to assessing educational needs of family medicine trainees in Ghana, we sought to assess whether those entering the training programme aimed to pursue an academic career.
Design A case study using an anonymous cross- sectional survey through collaboration between faculty members from the family medicine departments of Ghana and the University of Michigan.
Setting The family medicine postgraduate trainees and the most recent graduates in the three training sites, Accra, Kumasi and Mampong, as well as modular residents in Ghana served as the targeted participants during data collection between October and November of 2018.
Participants Second and third year family medicine residents, fellows (known as senior residents in Ghana) and recent graduates were invited to participate in this study. Thirty- five of 77 eligible subjects provided responses (46% response rate), but five records were eliminated due to incomplete data to yield a survey completion rate of 39% (30/77).
Result Participants were mostly men (n=19), and the average age of respondents was 37 years old. The participants indicated the residency programmes needed more faculty 97% (n=29), supervision during outpatient care 87% (n=26) and lectures 83% (n=25). The main reason provided by respondents for entering residency programme in family medicine, which is currently not required for practising primary care in Ghana, was to obtain more education 93% (n=28). Participants who had completed the residency programme were much more likely to be interested in becoming faculty compared with those still in residency (p <0.001).
Conclusion The research confirms the need for more faculty and the importance of investing in faculty development resources for ensuring a robust programme. These findings provide constructive feedback that could improve residency curricula of the local and regional family medicine training programmes and supports investing in trainees and new graduates as future faculty candidates.
INTRODUCTION
The richness of the family medicine disci—pline goes beyond its encompassing many aspects of other disciplines, because it is an approach where family physicians consider patients’ own values, their beliefs and envi—ronments while also collaborating with many specialists.12Leaders in healthcare in Africa are increasingly realising the importance of family physicians, especially for rural areas.3Family physicians are often the first contact for patients regardless of age, gender or religion. Global reports indicate there are disparities in cancer and non— communicable disease prevention, and therefore mortality, between low— income and middle— income countries and high— income countries.4Policy makers seeking an efficient health system need to focus on community health, a task adeptly handled by primary care physicians.
Developing a new residency programme in sub— Saharan Africa is a challenging under—taking, and its success is at least partially reliant on local and regional collaboration.5On one hand, main challenges are developing appro—priate and culturally customised curriculum as well as ensuring there are resources for its success.6On the other hand, comparisons between Ethiopia and the USA, Japan and the USA and from China, suggest that resident perspectives about fundamental training challenges in family medicine are more similar than dissimilar.7—9The residency programmes’ curricula periodically undergoes formal review and changes when the need arises, espe—cially when needs are expressed by the current trainees in the setting of dedicated, supportive and transparent faculty members. Residency programmes ideally should undergo some formal evaluation in order to be sure they are providing adequate teaching and supervision for trainees.10Residents are an important constituency as the training is designed for their development and their perspectives on training merit consideration.
The population in Ghana is ageing rapidly with a concomitant increase in complexity of medical care and chronic illnesses.11Previous research has shown there is limited care access for critical conditions such as stroke and large variability in the quality of care.12Chronic medical conditions such as hypertension, coronary artery disease and diabetes are prevalent, and the population faces access challenges for achieving delivery of high— quality care and preventive services.1314The success of Ghana’s health system is dependent on having qualified primary care doctors especially in rural areas.15Family physicians can handle the majority of the health needs of patients in rural districts. Moreover, they are crucial in tertiary centres where they can serve the primary care needs of the large population centres and serve as a gateway for specialists, a feature that contributes to cost effective care for the Ghanaian health system without compromising the quality of care.16Unfortu—nately, previous data suggest Ghanaians have much worse cardiovascular health compared with the European popu—lation.1718Additionally, research has shown that having a health system that allows access, awareness and educa—tion to diabetes and hypertension resources will improve the outcome of these illnesses.19While a system based on family medicine seems an obvious solution, family medi—cine faces a significant challenges.
In Ghana, medical school graduates can practice primary care once they complete a 2— year internship even without completing formal residency training programme in primary care afterwards. This is important first because there are many medical school graduates who opt to leave the country, despite the establishment of the Ghana College of Physicians and Surgeons and proac—tive efforts to retain medical school graduates.20Ghana needs to retain its medical school graduates to train and practice. Unfortunately, graduates increasingly have been leaving Ghana to practice in high— income coun—tries, though some opt to enter family medicine training programmes.2122While medical schools are proud of their emigrants’ achievements and success abroad, a national health priority is to retain these graduates and provide them with opportunity to progress in their career inside their home country.23In contrast to many high— income countries, medical student graduates in Ghana are licenced to work as clinicians after a 2— year internship as formal residency training is not required to practice. Among speculated reasons for why medical students chose to enter residency programmes is the extra training and supervision that they will obtain to support them when they practice independently. Pursuing such training abroad will potentially confer financial benefits and pres—tige. Engaging in teaching and scholarly activities could prove to be an appealing factor for enrolling in formal training programmes in the homeland. Given the need to minimise brain drain from Ghana and to retain medical school graduates for training in family medicine, research to better understand motivations of trainees who remain in Ghana for training in family medicine is needed.
While establishing a family medicine residency training programme in Ghana faces many challenges as in many other countries in sub— Saharan Africa, the need is great.524This is especially true in rural district hospi—tals of West Africa.2526Like many other sub— Saharan African countries, family physicians’ responsibilities in Ghana are evolving especially given advances in health—care, an increasing prevalence of chronic diseases, and an ageing population.27Family physicians’ roles differ substantially among physicians practising in the same country depending on whether they practice in urban versus rural areas.28Their potential varies based on where they completed their postgraduate training.29There is a good evidence to support the effectiveness of population health programmes and their role in improving commu—nity health in Ghana.3031Given the rise of chronic non— communicable diseases in Ghana, there is even more concern about the need for expansion as the available programmes are already inadequate to handle the need.32These circumstances further emphasise the need for family medicine residency training in Ghana.
The family medicine residency in Ghana started in 1999 and has experienced remarkable development with limited resources. Residents often need a sponsor who will financially support them during residency training. This is a critical issue because sponsored residents need to payback the financial support received by working for the sponsor after completing residency. This limits a resident’s ability to pursue an academic career in family medicine despite the dire need for faculty. The Ghana family medicine training programme has two compo—nents. The first is a 3— year training programme that can be initiated after completing the 2— year required internship. Residency graduates earn prestigious membership of the Ghana College of Physicians and Surgeons. Regarding the second, they can subsequently apply for an optional 2— year research— based fellowship (such a trainee is called a senior resident in Ghana and is comparable with a fellow in the US model). At the time of this research, there had been nearly 100 family medicine training programme graduates from the three training sites in Accra, Kumasi and Mampong. The fund for family medicine training in Ghana is primarily through the Ministry of Health, which receives its funds from the Ghanaian Government.
In Ghana, licenced medical officers may not undergo further formal training after internship. They are gener—alists who rise through the ranks by informal training and years of service. Medical officers do practice broad— spectrum primary care, but they gain different expertise depending on their location of practice and their years of practice. Family physicians with further formal training after internship are designated as specialists (after resi—dency) and senior specialists (after completing senior residency known as fellowship in US systems).
Practice scope, professional recognition and remuner—ation are therefore different for the two groups although they both work in primary care facilities.
The family medicine department at the University of Michigan, USA began collaborating with their Ghanaian colleagues in 2008 to support and sustain primary care education and research in Ghana. This collaboration has proven a productive one given extensive scholarly activi—ties and publications.33—39The collaboration has involved faculty exchanges between Michigan and Ghana. Faculty from the University of Michigan have provided lectures and supported the certifying examination process in Ghana. Ghanaian faculty have participated in research and faculty development in the University of Michigan. Moreover, the Department of Family Medicine at the University of Michigan helped coordinate a collabora—tion between the Geriatric Division of the University of Michigan and Department of Family Medicine in Ghana that fostered the establishment of the first training programme in geriatric medicine in Ghana.40These efforts not notwithstanding, there remains a need for adequate faculty development resources in Ghana to support faculty growth and their endeavours teaching and supporting their trainees.4142The critical need is for more faculty development resources that currently are both limited and challenging to access even when they become available.43
It is not well known what is needed for the programme success and sustainability and why medical school grad—uates would choose additional family medicine training when they can practice primary care after the 2— year internship. Moreover, information is lacking about how Ghanaian family medicine trainees view the teaching they receive and what teaching formats are needed most. Thus, we conducted research to understand current trainees’ and recent graduates’ views about their education and interest in teaching.
METHODS
Design
We conducted a case study design through use of an anon—ymous cross— sectional survey. The case study was bounded by the three residency programmes of the Ghana family medicine residency. The survey was designed using the Qualtrics survey platform in a collaboration between faculty from the family medicine departments of the Ghana College of Physicians and Surgeons and the University of Michigan.
Setting
The family medicine postgraduate trainees in the three training sites, Accra, Kumasi and Mampong, as well as modular residents in Ghana served as the targeted participants during data collection from October and November of 2018. Accra is the capital of Ghana and home to the country’s premier health facility, Korle— Bu Teaching Hospital, where the family medicine programme is located. Kumasi is the second largest city in Ghana, and the family medicine programme is also part of the teaching hospital, Komfo Anokye Teaching Hospital. The programme in Mampong is based in a large district hospital, the Tetteh Quarshie Memorial Hospital. A fourth training category of participants included was ‘modular residents’ who do their training in accredited ‘training complexes’. A training complex is a cluster of health facilities including rural district hospitals with affil—iated health centres and a regional hospital located in the regional capital.
Participants
Family medicine residents (PGY2 and PGY3), senior residents and the most recent residency graduates group (at the time of survey distribution) in September 2018 served as the targeted participants. First year residents were excluded since they had only been in the programme for 1 month at the time of survey distribution.
Data collection instrument
The survey was developed by faculty members of the Family Medicine Department of the University of Mich—igan (GT and MDF) in collaboration with chair of the Family Medicine unit in Ghana (AE). One of us (GT) visited eligible training sites in the fall of 2017 and met with faculty members and trainees to determine key constructs for inclusion in the survey. The authors designed the data collection instrument to assess the teaching of family medicine in Ghana from the trainees’ views. The primary constructs of measurement included four scales: reasons the trainee joined the programme (five items), trainees’ assessments of their education (eight items), the teaching strength of the programme (six items) and research opportunities (seven items). We further addressed modalities of learning used, perspectives on the partic—ipants’ future career and a general demographics ques—tionnaire. The items used 5— point Likert scale questions addressing their views of importance: 5=very important, 4=important, 3=moderately important, 2=little impor—tance and 1=unimportant, and agreement: 5=strongly agree, 4=agree, 3=neither, 2=disagree and 1=strongly disagree.
Data collection process
We recruited participants by emailing them a Qualtrics link to the survey which was available only for 60 days. Those who logged into the platform, read an informed consent statement and took the survey were consid—ered enrolled. It was distributed to each subject twice to maximise data collection. Data were collected between October and November 2018.
Data entry and statistical analysis
Participants directly entered their responses into Qual—trics. Their responses were downloaded from Qualtrics, and the dataset was managed using an excel sheet. The analysis was conducted using SAS (Statistical Analysis System) version 9.3 by a statistician at the University of Michigan. The primary outcome of the analysis was interest in academic career. Five— point Likert scale ques—tions about importance were reported by the distribution providing the response. Five— point Likert scale ques—tions about agreement were dichotomised as agree and neither/disagree responses. The study was reviewed and approved by the institutional review boards at the Univ—eristy of Michigan and the Ghanaian health institute especially given the fact it is anonymous survey with no to minimal harm to subjects.
RESULTS
Thirty— five of 77 eligible subjects provided responses (46% response rate), but five records were eliminated due to incomplete data that resulted in a survey comple—tion rate of 39% (30/77). Among 61 subjects in training during survey distribution (PGY2, PGY3 and senior resi—dents the latter who would be called fellows in US termi—nology), there were 23 subjects in Accra, 13 in Kumasi, 3 in Mampong and 22 who were modular residents. The remaining 16 subjects comprised the most recent gradu—ating cohort from September 2018 (academic year runs September—August). The mean age of the 30 participants providing information was 37 (SD=5) years, about the age expected as many medical school graduates have already gained work experience in primary care before entering residency. As table 1 indicates, there were almost twice as many male respondents as females (64% vs 33%). A mean of 5.7 (SD=5.2) years had elapsed between intern—ship completion and entering a residency programme.
Views on becoming family medicine faculty
Regarding interest in becoming a faculty member, as illus—trated in table 2, proportionately more men (13/19) than women (4/10) were considering work as a faculty member. As a group, a higher proportion (8/11) of those who had graduated from medical school within 4 years were favour—able to an academic path than those (7/14) who graduated from medical school 5 or more years prior. The vast majority of those responding (59% (16/27)) appreciated the impor—tance of research. Only 53% (16/28) showed an interest in becoming a faculty member. Among the training sites,proportionately, Kumasi and Mampong respondents were more likely to consider working as faculty though this was not statically significant. Participants who had completed a residency programme were much more likely to be inter—ested in becoming faculty when compared with those still in residency (p<0.001). When senior residents (equivalent to fellows in the US system) who had completed residency programme were lumped together with the recent grad—uates, the relationship remained statistically significant (p=0.002).

Table 1 Characteristics of the respondents
Motives for entering family medicine residency
Among motives for entering a family medicine training programme as depicted in table 3, ‘needing more educa—tion’ was the most important factor 93% (n=28). This was followed by passion for primary care and then procedural training. Only 23% (n=7) felt income was a big factor in their decision to join a residency programme. While not depicted in the table, 77% (n=23) felt the programme provided a high quality of teaching overall. This held true among the vast majority for the inpatient service 83% (n=25), but only 57% (n=17) of the respondents rated the teaching quality in the outpatient settings as ‘high’.
Views on potential areas of improvement
When asked what areas of residency training should be improved in the residency programmes, as demonstrated in table 4, 97% (n=29) of participants felt the programme needed more faculty members and that the residencies needed more outpatient supervision (87% (n=26). They indicated also more need for lectures 83% (n=25) as well as supervision in the inpatient setting 80% (n=24). Only a minority felt additional rotations were needed 40% (n=12).
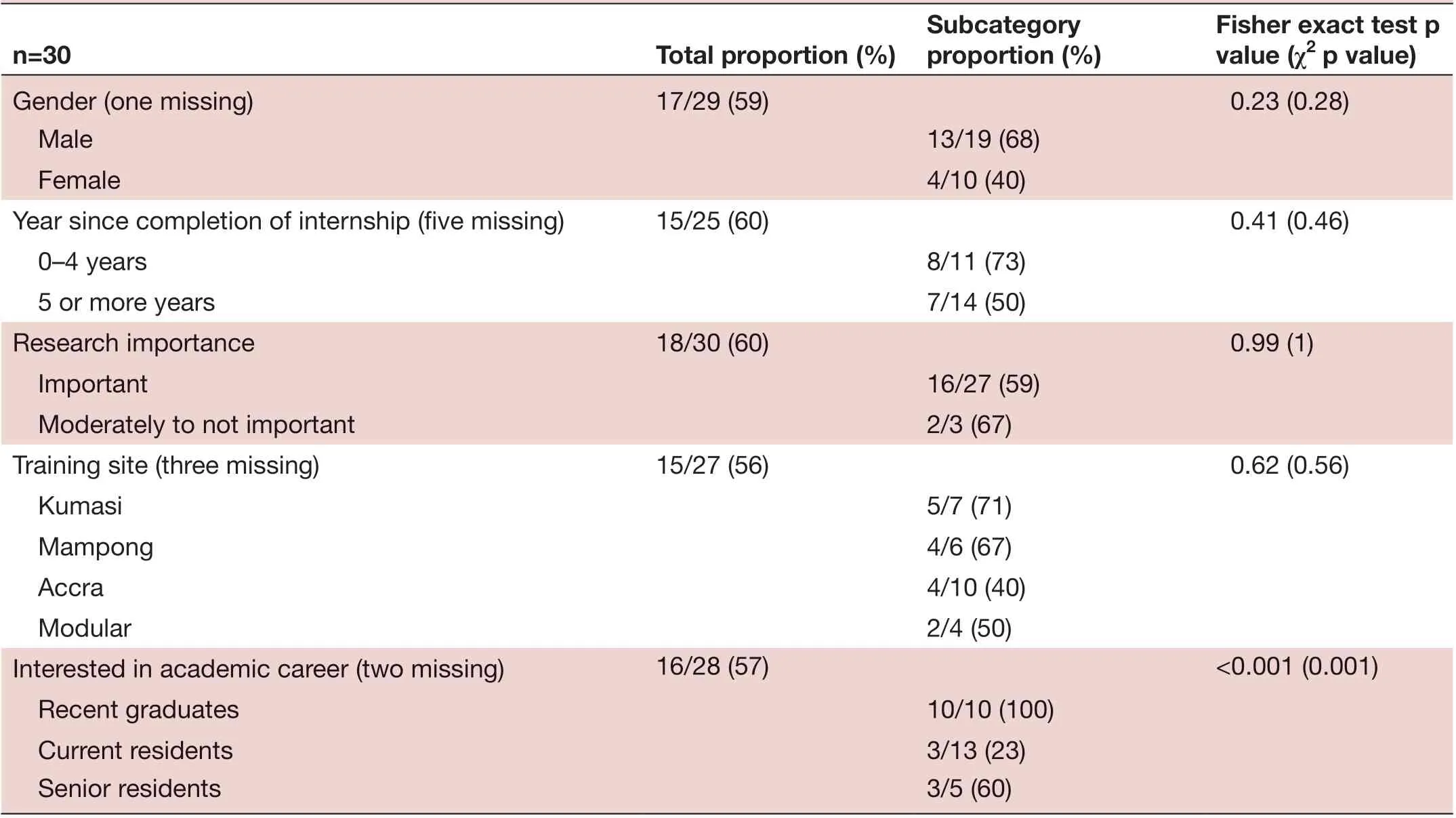
Table 2 Interest in academic career of the respondents based on age, year since graduation, training site, research interest and training level
Views about research, faculty and programme resources
As shown in table 5, the participants identified a lack of resources (90% (n=27)), research mentorship (77% (n=23)) and their own research knowledge (73% (n=22)) as the main barriers for research. Regarding perceptions about faculty as illustrated in table 6, 93% (n=28) had a positive impression of the professionalism of faculty. Also, 73% (n=22) of respondents felt positively about faculty being knowledgeable, caring about resident education and communicating well. In reference to the most frequently accessed learning sources as presented in table 7, the participants reported most heavily relying, that is over 15 times per month, on online (40% (n=12)) and book sources (37% (n=11)). As shown in table 8, the respondents indicated that the case studies, small group discussions and books were the main learning modalities provided by the programme. However, 73% (n=22) of respondents felt the programme is lacking online materials, and 63% (n=19) of respondents felt the programme is lacking simulation materials.
DISCUSSION
This is the first known assessment by trainees of the quality of their family medicine residency in this region. As data collection occurred external to the residency infrastruc—ture, we assert the findings as important for being trans—parent relative to the views of the participating residents. In previous work on the continent in South Africa, a training physician portfolio was found to have a posi—tive educational impact of family medicine trainees, but the research also revealed a lack of assessment skills and feedback by the faculty.44The ability of faculty to provide feedback to trainees is critical for advancing the trainees’ career advancement. We anticipate data from this study could help guide thinking about educational content inGhana and evaluation opportunities for other training programmes in primary care in other parts of West Africa. Such an assessment can also inform curriculum development. These findings highlight the importance of primary care training as well as needs for Ghana.45—48In light of these findings, the department has expanded and now there is a fourth residency site.

Table 3 Motivations for entering family medicine by respondents
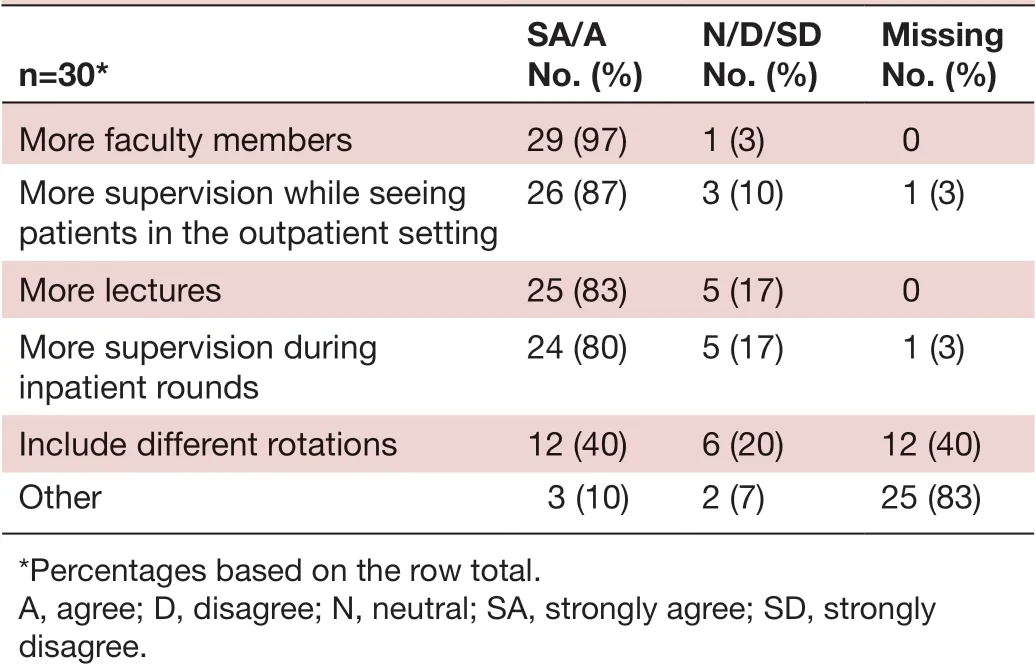
Table 4 Opportunities for improving the family medicine programme’s teaching
Addressing the shortage of faculty
These findings confirm observations by the Ghanaian family medicine leadership and the US physician (GT) who visited Ghana that the main challenge in primary care training is the shortage of faculty. Unexpectedly, the survey revealed that during residency, participants did not feel practically interested in pursuing an academic career. However, after completing residency programme, graduates were much more inclined to do so, a statisti—cally significant finding. A plausible explanation is that those who finish residency could be missing the joy of academia. Also, those still in residency training might feel overwhelmed with learning to be a clinician or may lean towards private practice since the latter is financially more rewarding. It is crucial to retain graduates of the

Table 5 Barriers to research according to the family medicine trainees and recent graduates
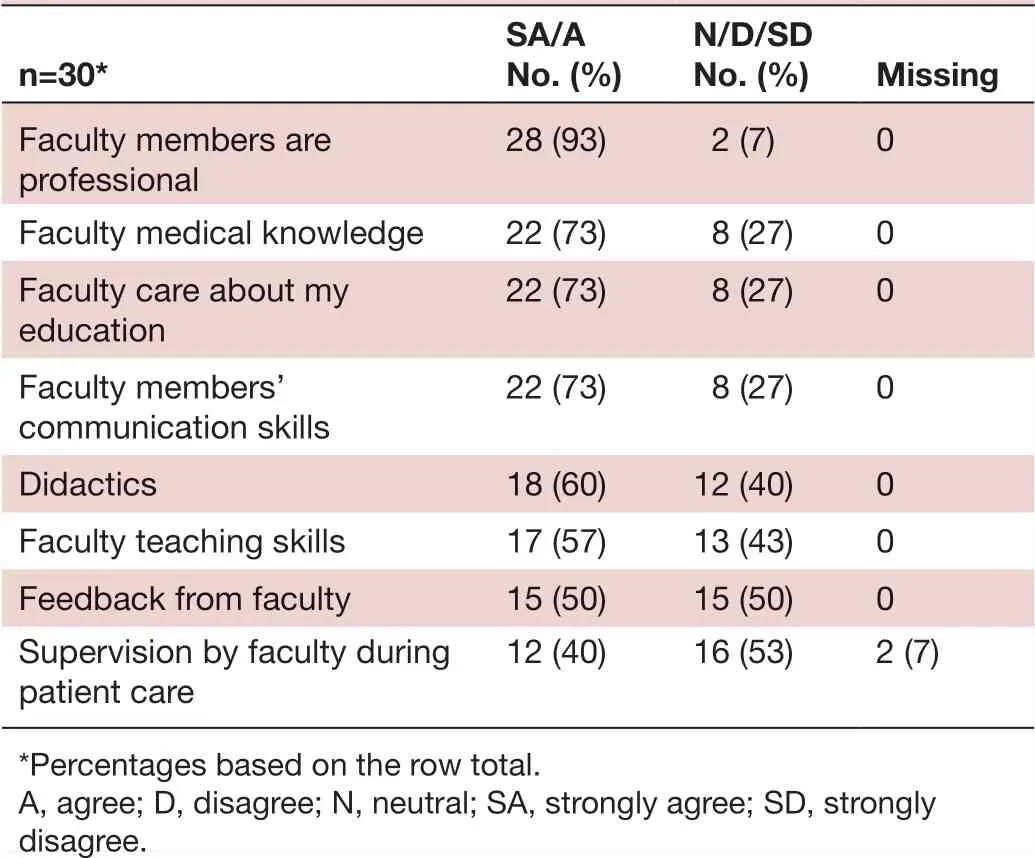
Table 6 Perceptions of faculty by family medicine trainees and recent graduates
programme to create the next generation of family medi—cine teachers in Ghana. Therefore, we suggest better reimbursement models and faculty development for trainees. These findings also revealed that the trainees are passionate about learning. The need for more educa—tion was the most commonly reported motive to join a residency programme, more so than improved financial reimbursement. Despite rating inpatient training as of a high quality, the respondents felt the need for more supervisoin in the outpatient as well as in the inpatient settings. Therefore, it is important to have more faculty as well as faculty development programmes. This would justify applying for grants outside Ghana that could help train residents in an academic track. The research instru—ment developed for this study could be used by other programmes to assess their performance from trainees’ perspective and provide comparison data.
Implications for addressing medical student outmigration
As chronic illnesses are increasing in prevalence among the Ghanaian population and sub— Saharan Africa, there is even greater urgency to produce high— quality primary care doctors to manage the healthcare needs of the general and ageing population. Family medicine is the best avail—able solution to handle the challenges related to compre—hensive care and the rise of chronic illnesses. Developing an attractive education curriculum is greatly needed to attract medical students and to help them formulate their specialty decision and future plans. We hope the use of these data will enhance the strength of the teaching programme by having a clear mission that will, in turn, help attract more medical school graduates to join family medicine training. Developing a robust and manageable curriculum is core to this mission. Research in Ghana has shown that the majority of medical students were appre—ciative of the work of family medicine but few had a good understanding of the specialty. The lack of understandingof family medicine appears to be a barrier for students to choose it as their preferred specialty.3349Ghana has one of the largest medical school graduates in West Africa with approximately 500 graduates per year. Therefore, effective collaboration between residency programme directors and medical schools could help positively raise awareness among medical students and attract them to join family medicine training. For example, direct entry after completion of the Ghanaian compulsory internship (which is required for entering residency) could help mitigate the loss of medical students to other countries. The structure and enhancements to the residency curric—ulum will enhance the ability of medical students to better understand their training opportunities in family medi—cine and to better formulate their decision to enter one of their training sites.50While published data are lacking, there is a general consensus among the Ghanaian family medicine leadership that primary care physicians trained in formal residency programmes provide superior patient care compared with those who have not completed a formal residency programme. Experience from China, which has been transitioning from a shorter training period to a longer training period, suggests other policy makers have reached the same conclusion about the value in training over a longer period of time.951
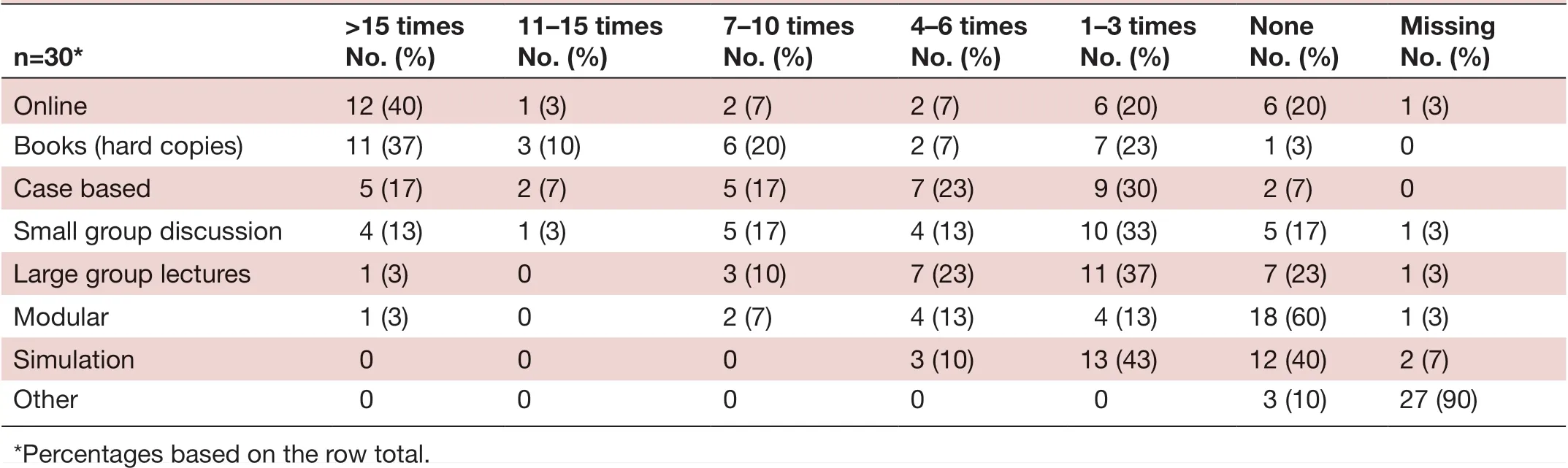
Table 7 Frequency of training modalities accessed by trainees in the family training programme
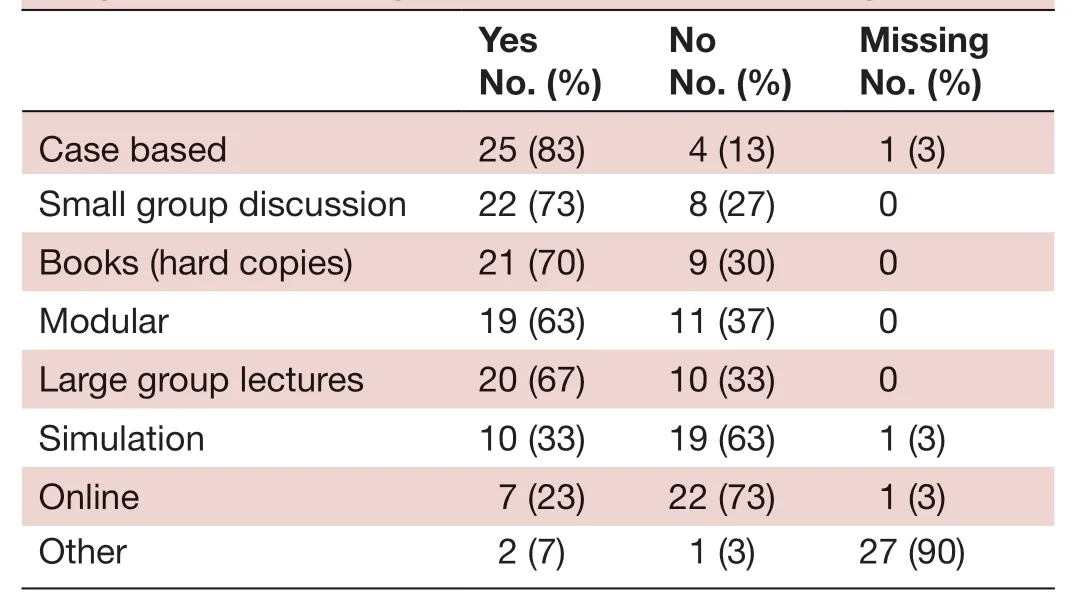
Table 8 Available training modalities provided by the programme according to the trainees and recent graduates
Study limitations
The primary limitation of this survey is the relatively low response rate. While caution is needed in generalising these opinions, the voices of the responding residents are real, and we have endeavoured to fairly represent them. Importantly, there were roughly similar proportions of respondents from all three sites operating at the time of the survey. Additionally, there is face validity between these results and observations on the ground and discus—sions between the US consultant (GT) and Ghanaian senior faculty (AE and others) during the preparatory phase of the study. Arguably, the residents’ least satisfied with their training would be the least likely to respond. However, we have good reason to believe the low response rate was due in part to logistical issues. First, the survey was only distributed twice during a 60— day period, which was also during the beginning of the busy new academic year. Some of the eligible subjects may have either missed the email invitation (handled as junk mail by their own email systems) or the survey link expired before they had time to complete their responses. This appears to have been the case for at least five incomplete records that were dropped from analysis. Second, the people of Ghana often experience inconsistent internet connec—tivity. Third, trainees used their own personal emails that are offered through commercial providers and not supported by a residency programme— associated service. Fourth, the US investigator directly emailed the survey link to trainees/graduates to mitigate concern that their responses could be viewed by the programme leadership and potentially result in retribution, but the unknown source could have been problematic as some residents would not be familiar with him.
CONCLUSION
Having qualified primary care doctors especially in rural areas is critical for the success of Ghana’s health system. This feedback from family physicians— in— training and recent graduates provides a window for understanding educational needs based on the perspective of trainees. These findings provide a perspective for both local and regional family medicine teachers for evaluating the residency curriculum. The survey findings emphasise the importance of investing in the programmes’ current trainees and graduates in order to recruit them into academic roles. Addressing the shortage of faculty appears to be a major challenge to sustaining the family medicine training programme in Ghana. As trainees indicate a rela—tive paucity of educational resources and too few faculty, more government funding is needed. In addition to more online resources, lectures and faculty supervision, strate—gies are needed to retain residency graduates to become future teachers equipped with faculty development experience. Making changes to enhance training could help make family medicine more attractive to medical school graduates. Ultimately, increasing student interest in family medicine is needed to expand the family physi—cian workforce and address the primary care physician shortage. Beyond the borders of Ghana, the survey could be used in other settings to acquire programme— specific information.
TwitterMichael D Fetters @mdfetters
ContributorsGT participated in study and survey design, data collection, analysis and manuscript writing. AE participated in study and survey design, and manuscript writing. MDF participated in study and survey design, data analysis and manuscript writing.
FundingMDF participation in this research was made possible through the Mixed Methods Program as supported by the Department of Family Medicine, University of Michigan. All participants provided informed consent for this study.
Competing interestsNone declared.
Patient consent for publicationNot required.
Ethics approvalThis study was approved by the institutional review board (HUM00144881) and the Ghanaian Health Institute.
Provenance and peer reviewNot commissioned; externally peer reviewed.
Open accessThis is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY- NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non- commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non- commercial. See: http:// creativecommons. org/ licenses/ by- nc/ 4. 0/.
ORCID iDsGhazwan Toma http:// orcid. org/ 0000- 0001- 6836- 7587 Akye Essuman http:// orcid. org/ 0000- 0002- 0784- 1123 Michael D Fetters http:// orcid. org/ 0000- 0001- 8521- 5681
 Family Medicine and Community Health2020年4期
Family Medicine and Community Health2020年4期
- Family Medicine and Community Health的其它文章
- Perceived barriers and primary care access experiences among immigrant Bangladeshi men in Canada
- The process of transprofessional collaboration: how caregivers integrated the perspectives of rehabilitation through working with a physical therapist
- Reformulation and strengthening of return- of- service (ROS) schemes could change the narrative on global health workforce distribution and shortages in sub- Saharan Africa
- New hypertension and diabetes diagnoses following the Affordable Care Act Medicaid expansion
- How well did Norwegian general practice prepare to address the COVID-19 pandemic?
- Exploring the structure of social media application- based information- sharing clinical networks in a community in Japan using a social network analysis approach