
Preoperative nuclear stress testing in the very old patient population
2020-06-12 08:57:02AmgadMakaryusJohnMakaryusJosephDiamond
World Journal of Cardiology 2020年5期
Amgad N Makaryus, John N Makaryus, Joseph A Diamond
Abstract
Key words: Pharmacologic nuclear stress testing; Prognosis; Elderly; Preoperative assessment; Outcomes
INTRODUCTION
The overall prognostic utility of both treadmill and pharmacologic stress testing is well established[1-4]. However, the utility of stress testing in those ≥ 85 years old is not well established. Octogenarians and nonogenarians typically have an elevated rate of coronary artery disease. Furthermore, to our knowledge no prior study has specifically examined the utility of nuclear stress testing (NST) with respect to surgical outcomes in the ≥ 85 years old age group. Thus, the prognostic value of nuclear stress testing for preoperative risk assessment has been questioned in this patient population.
In the present study, we sought to determine whether results of indicated preoperative nuclear stress tests (NST's) have prognostic value in predicting perioperative and post-operative cardiac events (one or more, none) in elderly patients undergoing moderate to high-risk surgery.
MATERIALS AND METHODS
Patient selection
We performed a retrospective descriptive study of 69 patients ≥ 85 years of age who underwent pre-operative nuclear stress testing (Figure 1). Patients undergoing lowrisk surgery as defined by the American College of Cardiology/ American Heart Association guidelines[5]were excluded. Other exclusion criteria were patients aged less than 85, and patients undergoing resting nuclear perfusion studies (i.e., viability studies).
Stress testing
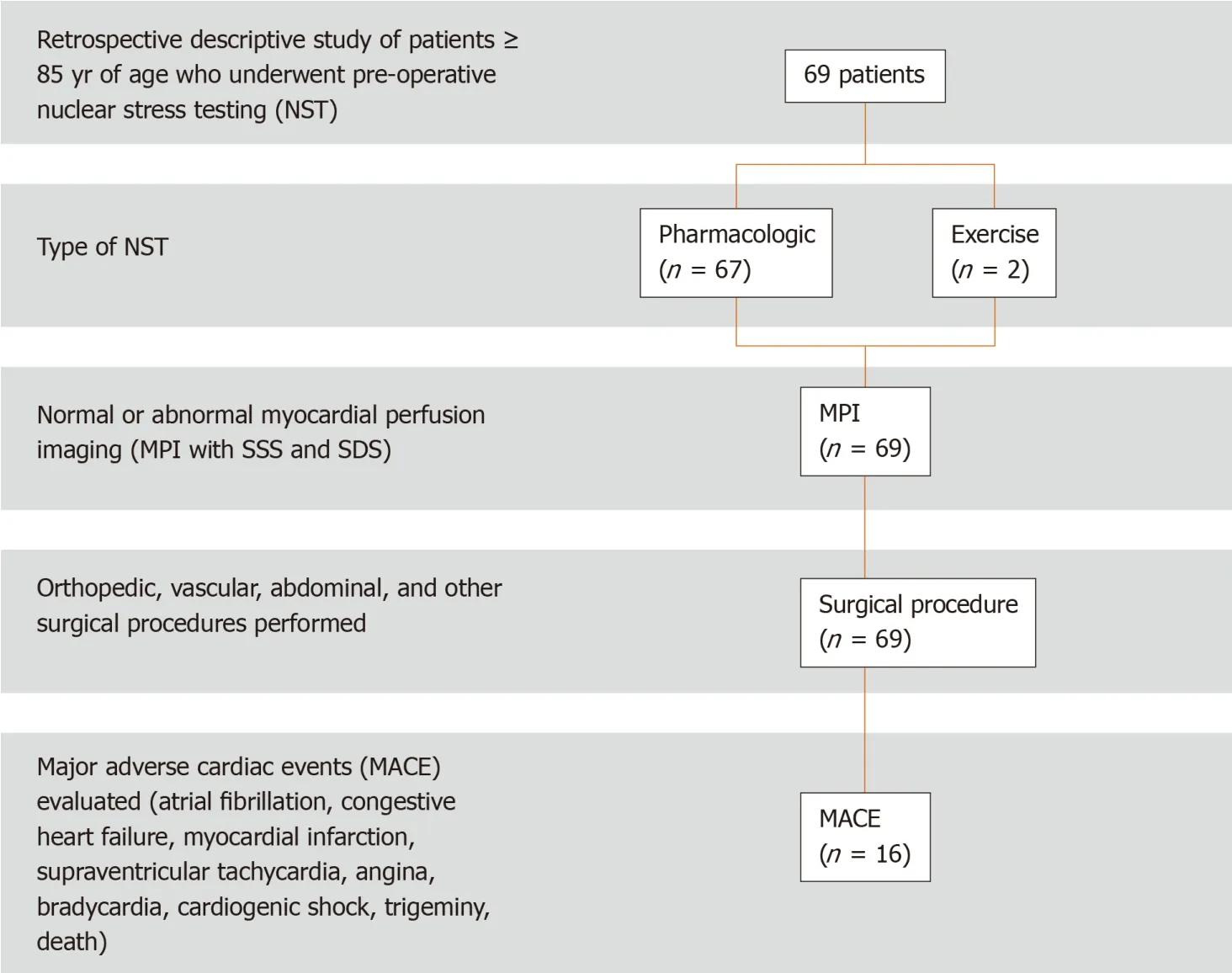
Figure 1 Study population flow chart. SSS: Summed stress score; SDS: Summed difference score.
Either pharmacologic (n= 67) or exercise treadmill stress testing (n= 2) was employed. An intravenous line was inserted prior to the start of the test. Exercise testing patients underwent symptom-limited treadmill exercise testing using a standard Bruce protocol. Heart rate, blood pressure, and 12-lead electrocardiograms were recorded before (supine and upright positions) and during each minute of exercise and recovery. Patients exercised until the point of fatigue unless marked electrocardiographic abnormalities, hemodynamic instability, chronotropic incompetence, ventricular tachycardia or fibrillation, or disabling chest pain symptoms occurred. Exercise was discontinued if exertional hypotension, malignant ventricular arrhythmias, marked ST depression, or limiting chest pain occurred. An abnormal electrocardiogram was defined as ≥ 1 mm ST depression.
In the pharmacologic testing patients, adenosine or dobutamine pharmacologic stress was performed. Adenosine was infused intravenously, at a dose of 140 mcg/kg per min over 6 min, with an administration of the radiopharmaceutical at the midpoint of the infusion. If patients exhibited persistent side effects from the adenosine, 75-125 mg of aminophylline were administered intravenously as needed.Dobutamine was infused using standard incremental dosing from 5-40 mcg/kg per min during which patients remained under continuous clinical, and electrocardiographic monitoring. Test endpoints included completion of the final stage of the protocol, severe ischemia (severe angina, > 2 mm ST depression),hypertension (systolic blood pressure > 220 mmHg), hypotension (drop in systolic blood pressure > 20 mmHg), arrhythmias, or side effects intolerable to the patient.Atropine (1 mg IV) was administered in patients who failed to attain 85% of agepredicted maximal heart rate at peak dose.
Myocardial perfusion imaging
Single photon emission computed tomography (SPECT) was performed at one institution (Long Island Jewish Medical Center) using one or two-day single-isotope protocols, employing either99mTc-sestamibi or99mTc-tetrofosmin. At our other site(North Shore University Hospital), a dual isotope (201Tl and99mTc-sestamibi) one-day protocol was employed. The myocardial single-photon emission computed tomography perfusion image acquisition was acquired at rest and after peak stress using a dual head Optima NX gamma camera at one site and a dual-head Millenium gamma camera (General Electric, ? Milwaukee, WS, United States) at our other respective site. The images were processed using standard commercial software(Pegasys?, Milwaukee, WS, United States). All SPECT acquisitions were acquired at rest and after peak pharmacologic stress using a circular orbit (180°), in a 64 × 64 matrix. Image processing was performed in a standard manner. All image sets(horizontal and vertical long-axis and short-axis planes) were normalized to the maximal myocardial activity in that set and displayed in the standard American College of Cardiology orientation. An experienced observer blinded to clinical outcome data reviewed all scans. Stress images were compared with rest images. A 20-segment scoring system that uses 3 short-axis slices [distal (apical), mid, and basal]of the left ventricle, with the apex represented by 2 segments visualized on a midvertical long-axis image was used. Each segment was scored as follows: 0 =normal, 1 = slight reduction of uptake, 2 = moderate reduction of uptake, 3 = severe reduction of uptake, and 4 = absence of radioactive uptake.
Adverse cardiac Events
A major adverse cardiac event (MACE) was considered for any adverse event that occurred prior to post-operative discharge. MACE included arrhythmia, myocardial infarction, unstable angina, heart failure, or death. The associations between patient risk factors, MACE, and the results of the pre-operative NST [normal (nl), abnormal(abnl)], the ejection fraction (EF < 40% or ≥ 40%), summed stress score (SSS ≤ 8, ≥ 9),and the summed difference score (SDS ≤ 0, > 0) were examined.
Statistical analysis
The use of logistic regression to examine the multivariate effects of nuclear stress test results and presence of cardiac risk factors prior to admission on intraoperative cardiac events (one or multiple) was undertaken. A Cox proportional hazards regression analysis was used to examine the multivariate effects of nuclear stress test results, presence of cardiac risk factors prior to admission and intraoperative cardiac events on time until first post-operative cardiac event.
In the analysis of in-hospital adverse events, it is generally felt preferable to use survival methods; we therefore examined length of stay since patients staying longer are more likely to have events regardless of other risk factors. However, because this was a retrospective chart review, it was not possible to obtain the dates of all events with certainty. Therefore, rather than deleting patients from the analysis, the analysis was carried out without regard to time. In order to examine the association between length of stay and stress test result, we estimated length of stay (LOS) using the product limit method, and compared LOS stratified by stress test results using the log rank test only for those patients not having an event in hospital. Presumably, any difference in LOS would then be due to the test result and not the occurrence of an adverse event. Similar analyses were carried out for ejection fraction, summed stress score, and summed difference score.
RESULTS
Clinical characteristics and stress test results
From the group of 69 patients (mean age 88 ± 2.6 years, 31 males) who underwent NST prior to surgery, Table 1 highlights the study population demographics. A majority of the patients had hypertension (82.6%) and 33.3% had hyperlipidemia.Abnormal NST was found in 60% (41/69) of the patients. A majority of the patients(37.7%) underwent orthopedic procedures followed by vascular surgeries (21.7%) and abdominal surgeries (21.7%).
Adverse cardiac events and in-hospital outcomes/mortality
Sixteen (23%) patients suffered post-operative MACE. Adverse events are detailed in Table 2. No significant associations were noted between risk factors and MACE (Table 3). Patients with an abnormal NST and/or an SSS ≥ 9 were significantly more likely (P< 0.02) to develop peri-operative MACE (Table 4). Patients with an abnormal stress test were 6.3 times more likely (P< 0.03) than those with a normal test to have a MACE prior to discharge (95% confidence interval: 1.3-30.5). Those with an EF < 40%or SDS > 0 (denoting ischemia) did not each show a statistical significance to developing peri-operative MACE, although in those with an EF < 40%, there was a trend toward significance with aPvalue of 0.065. Figure 2 shows the example of a patient who suffered post-operative heart failure after hip fracture repair. The images reveal an area of infarct in the proximal inferolateral wall with ischemia in the mid to distal inferolateral wall. A SSS of 22, and a SDS of 7 were noted in this patient.
DISCUSSION
Our investigation adds significant information to the body of evidence that shows prognositic utility of both treadmill and pharmacologic stress testing, but it adds this information in the population of octogenarians and nonagenarians who were underrepresented in many of the landmark prognostic evaluations of NST. Furthermore, no prior study has specifically examined the utility of NST with respect to surgicaloutcomes in the ≥ 85 year old age group. This information is useful as it is not uncommon for these patients to undergo surgical operations, particularly orthopedic procedures. We found that clinical underlying risk factors did not predict outcomes.This is an important finding as many of these patients are sent to surgery without prior further stratification aside from risk factor assessment and modification. Also,although the SSS was a significant predictor of MACE, the SDS and the EF were not.This may be due to the small sample size as there is a trend in thePvalues towards significance. Prior studies[1,2]support the fact that the SSS is the major predictor of adverse events as opposed to the SDS. The NST, specifically an abnormal nuclear perfusion result and/or a SSS ≥ 9 (severely abnormal study), identified those patients significantly (P< 0.01) more likely to develop peri-operative MACE.

Table 1 Patient demographics
Few prior investigations have examined the question of the prognostic utility of NST in the very elderly (≥ 85) age group[6-15]. Although these studies demonstrate the utility of NST in the elderly for predicting cardiac events, they do not focus on the specific situation of pre-operative risk assessment; our study does. Another discrepancy in these studies is the age cutoff for an “elderly” patient. Some authors ascribe an “elderly” patient to the ≥ 55 years range[13], while others use the cutoff of ≥65 years[6,11,12], ≥ 70 years[14,15], ≥ 75 years[9], or even ≥ 80 years[7,8,10]. Our study specifically assessed prognostic outcome after moderate-to high-risk surgery in patients ≥ 85 years, thus targeting a special population of very elderly individuals.
In the evaluation by Steingartet al[6], the clinical, electrocardiographic (ECG) stress test, NST, and follow-up data for 626 patients aged ≥ 65 years (mean age 70 ± 4.4) with interpretable electrocardiograms undergoing symptom-limited exercise NST between 1992 and 1996 were evaluated with follow-up occurring after 4.4 ± 1.3 years. They found that the following factors predicted death or myocardial infarction: Male sex,increasing age, an abnormal rest ECG result, lower exercise tolerance and lower peak exercise heart rates, exercise ST-segment depression, left ventricular dilatation, and the number of ischemic regions. After multivariable analysis, only increasing patientage, male sex, limitation of exercise tolerance, and the number of ischemic segments by NST were predictive of death or myocardial infarction. They concluded that in elderly patients undergoing exercise NST, age, sex, exercise tolerance, and ischemia on NST provide significant prognostic information in this patient population. Nuclear imaging provided incremental prognostic information that was significant in comparison to clinical information and results of exercise testing[6].
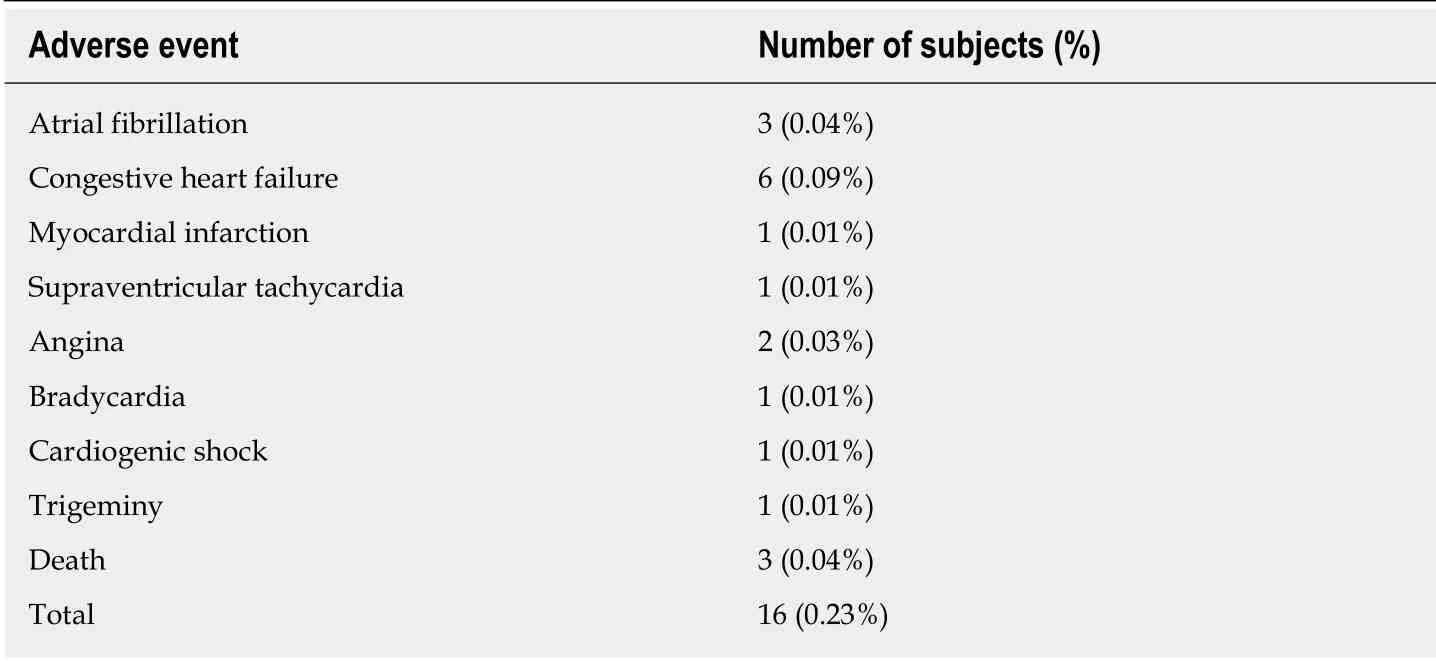
Table 2 Major adverse cardiac events
Gorayaet al[11]assessed treadmill exercise testing in an elderly population (≥ 65 years of age) to evaluate the incremental value of the testing to clinical data. A comparison was undertaken with a median follow-up of 6 years with results of treadmill testing in younger patients (< 65 years). Elderly patients, as compared with younger patients, had more comorbidities, achieved a lower workload (6.0vs10.7 metabolic equivalents;P< 0.001), and had a greater likelihood of an abnormal exercise ECG (28%vs9%;P< 0.001). Overall survival (63%vs92%;P< 0.001) and cardiac event-free survival (66%vs95%;P< 0.001) were worse among the elderly persons.The amount of workload achieved was the only treadmill exercise testing variable associated with all-cause mortality (P< 0.001) in both age groups. Workload was also the only additional treadmill exercise testing variable that was predictive of cardiac events (P< 0.05). Notably, each one metabolic equivalent rise in exercise capacity was associated with a 14% and 18% reduction in cardiac events among younger and elderly persons, respectively. They conclude that in elderly persons, treadmill exercise testing provided incremental prognostic information that was significant and incremental in comparison to clinical information. ECG results of stress testing (e.g.,the presence of ST-segment depression) was likely not a significant contributor to prognosis, because in the elderly there is a higher occurrence of resting (baseline) STsegment changes and higher use of medications that may cause falsely positive ECG changes. Exercise workload on the treadmill was the only variable that was strongly associated with outcome, and its prognostic effect was equal in both the young and elderly age groups[11].
A report by Zafriret al[8]examined 162 consecutive patients (mean age 83 ± 3 years)who underwent NST with a duration of follow-up of 45 ± 12 months. Nineteen percent of patients (31) had major cardiac events recorded; including 26 cardiac deaths and 5 MI events, in 6 of the 61 women (10%) and 25 of the 101 men (25%) (P<0.03). The univariate predictors of cardiac death or MI, aside from known coronary artery disease (CAD), included NST variables such as left ventricular dilatation,increased lung uptake, abnormal scan, and the presence and extent of myocardial ischemia. The only predictors for major cardiac events, however, were: left ventricular(LV) dilatation (OR = 6.9, 95%CI: 2.7-17.4,P< 0.0001) and ischemia by scan (OR =2.75, 95%CI: 1.09-6.96,P< 0.03). Survival curves demonstrated significant differences in survival between patients with or without LV dilatation and patients with or without ischemia. They conclude that in octogenarian patients with CAD or with suspicion of CAD, LV dilatation and myocardial ischemia are useful predictors of cardiac death and MI[8].
A report by De Winteret al[9]further used not only perfusion imaging in the prognostic assessment of elderly patients, but adds left ventricular function analysis as a further criterion in the evaluation. The clinical and gated SPECT predictors of cardiac and all-cause death in 294 patients aged ≥ 75 years with known or suspected CAD who were referred for tetrofosmin cardiac gated SPECT imaging were examined. During a median follow-up of 25.9 months, a total of 47 patients (16%)died. In their multivariate Cox proportional hazards regression analysis, the summed rest score, transient ischemic dilatation index, and resting left ventricular ejection fraction were independent predictors of all-cause death. The summed rest score and resting end-systolic volume were independent predictors of cardiac death. They conclude that NST left ventricular functional data assessed during myocardial gated SPECT provides independent and incremental information above clinical and perfusion SPECT data for the prediction of cardiac and all-cause death in patients aged ≥ 75 years[9].
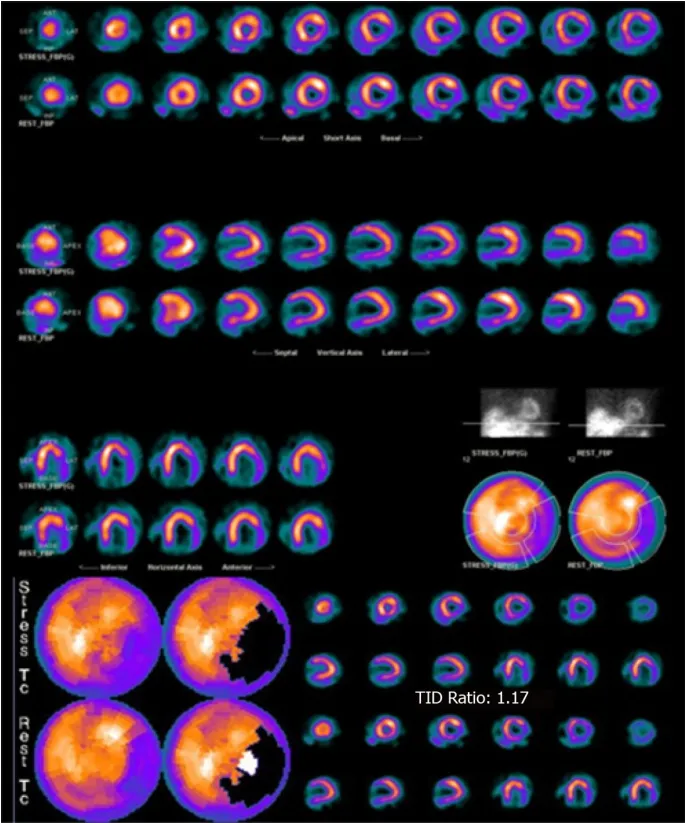
Figure 2 This image shows the nuclear stress testing result of one of our patients: An 88 year old man who presented with a fracture of his left hip. He was risk stratified by undergoing adenosine pharmacologic nuclear testing. The images reveal an area of infarct in the proximal inferolateral wall with reversibility (ischemia) in the mid to distal inferolateral wall.
Study limitations
The relatively small sample size of the study group limits our study findings. The small number of post-operative MACE is also a limitation, but may just be a credit to our advancing health-care techniques in the peri-operative period. Additional study of larger numbers of individuals would allow more specific analyses of NST's. For example, prognosis may be stratified by different categories of summed stress scores.Another limiting factor is that our analysis only included those patients who underwent surgery. It is not unreasonable to surmise that many patients who had abnormal NST might have had their surgeries cancelled due to their assumed high risk. This may introduce referral bias into the analysis, with potential for decreasing the correlation between abnormal studies and unfavorable surgical outcomes. It is also assumed that certain surgical techniques may have been modified as a result of the findings on NST.
In the analysis of in-hospital events, it is generally preferable to use survival methods, so that length of stay is considered, since patients staying longer are more likely to have events regardless of other risk factors. Since this was a retrospective chart review, and it was not possible to obtain the dates of all events with certainty,rather than deleting patients from the analysis, we carried out the analysis without regard to time. However, if there were an association between risk factor and length of stay, then this analysis would be biased, since patients with a longer stay would be more likely to have experienced an event simply because they were in the hospital longer. On the other hand, patients experiencing an event may have longer stays as a result of the event. Therefore, in order to examine the association between length of stay and stress test result, we estimated length of stay (LOS) using the product limit method, and compared LOS stratified by stress test results using the log rank test only for those patients not having an event in hospital. Presumably, this way any difference in LOS would then be due to the test result and not the occurrence of an adverse event. Similar analyses were carried out for ejection fraction, summed stress score, and summed difference score. These analyses showed no associations between any of the test results and LOS for subjects not having an in hospital event.
In conclusion, the use of nuclear stress testing is a useful tool to assess preoperative risk and post-opertive outcome stratification in elderly patients ≥ 85 years undergoing moderate to high-risk surgery in whom the test is indicated based on latest preoperative risk stratification guidelines. In a time when recommendationsnow tend to less commonly recommend pre-operative testing, because the prediction of the development of post-operative complications using NST is possible, the use of NST in the appropriate patients should yield important and applicable information for it to benefit the patient and affect management. As our study demonstrates, an abnormal NST, and more specifically a significantly abnormal study with SSS ≥ 9, was noted to be highly predictive for the development of MACE in the immediate operative period in elderly patients ≥ 85 years undergoing moderate to high-risk surgery.
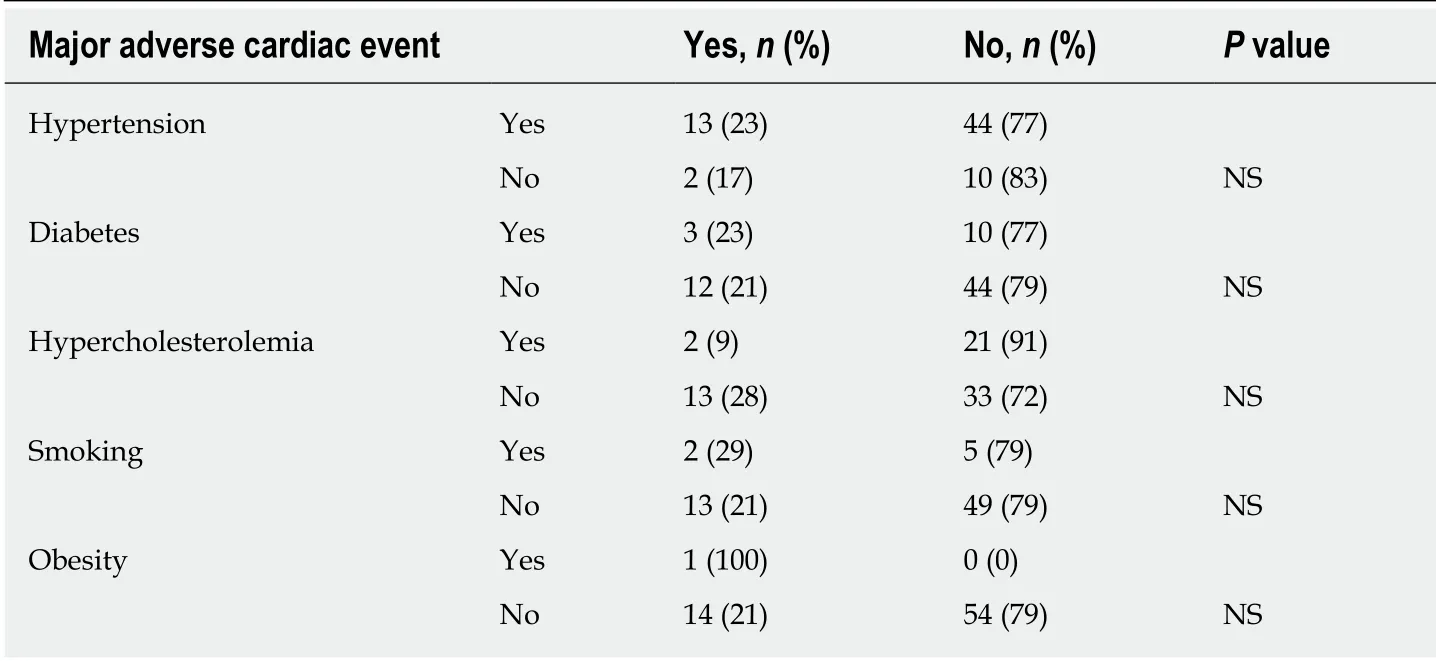
Table 3 Major adverse cardiac events and risk factors
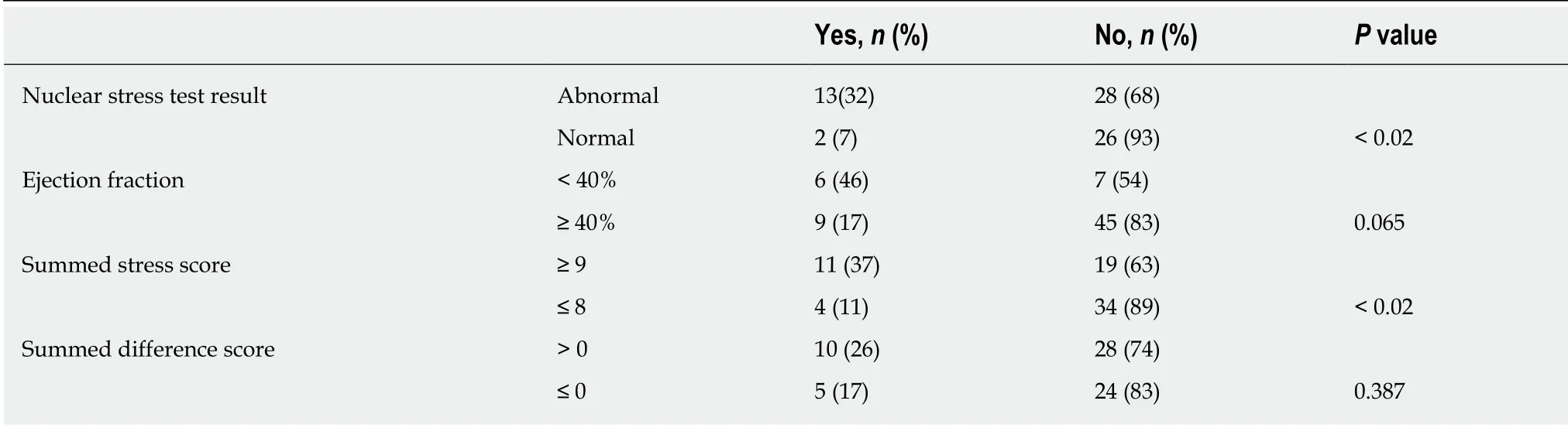
Table 4 Major adverse cardiac events and nuclear stress test variables
ARTICLE HIGHLIGHTS
Research background
It is common for elderly patients awaiting moderate to high-risk surgery to undergo nuclear stress testing in order to evaluate their cardiovascular risk. However, the prognostic utility of such testing in the very elderly (≥ 85 years) has yet to be evaluated.
Research motivation
The very elderly (octogenarians and nonagenarians) frequently have a number of concurrent conditions in addition to a high rate of coronary disease and therefore the prognostic value of nuclear stress testing for their preoperative risk assessment has been questioned.
Research objectives
We sought to assess the ability of nuclear stress testing to predict peri-operative cardiac outcomes in these patients.
Research methods
We undertook a retrospective descriptive study of 69 patients ≥ 85 years of age who underwent pre-operative nuclear stress testing. Patients undergoing low-risk surgery as defined by guidelines were excluded. Other exclusion criteria were patients aged less than 85, and patients undergoing resting nuclear perfusion studies (i.e., viability studies).
Research results
We found that there were no significant associations between risk factors and major adverse cardiac events (MACE). Patients with an abnormal nuclear perfusion result and/or a summed stress score ≥ 9 were significantly (P< 0.01) more likely to develop peri-operative major adverse cardiac events.
Research conclusions
Indicated nuclear stress testing is useful to assess pre-operative risk in elderly patients ≥ 85 years undergoing moderate to high-risk surgery.
 World Journal of Cardiology2020年5期
World Journal of Cardiology2020年5期
- World Journal of Cardiology的其它文章
- Management of hypertension in COVID-19
- Incidental discovery of right ventricular lipoma in a young female aImaging investigations and diagnosissociated with ventricular hyperexcitability: An imaging multimodality approach
- Access to smart devices and utilization of online health resources among older cardiac rehabilitation participants
- Nicotine-induced adrenal beta-arrestin1 upregulation mediates tobacco-related hyperaldosteronism leading to cardiac dysfunction
- Management of adults with coarctation of aorta
- New guidelines for the diagnosis and management of pulmonary embolism: Key changes