
Comparison of sentinel lymph node detection performances using blue dye in conjunction with indocyanine green or radioisotope in breast cancer patients: a prospective singlecenter randomized study
2018-12-07 06:21:40LongYuanXiaoweiQiYiZhangXinhuaYangFanZhangLinjunFanLiChenKongyongZhangLingZhongYanlingLiSijieGanWenyingFuJunJiang
Cancer Biology & Medicine 2018年4期
Long Yuan, Xiaowei Qi, Yi Zhang, Xinhua Yang, Fan Zhang, Linjun Fan, Li Chen, Kongyong Zhang, Ling Zhong,Yanling Li, Sijie Gan, Wenying Fu, Jun Jiang
Department of Breast Surgery, Southwest Hospital, Third Military Medical University (Army Medical University), Chongqing 400038, China
ABSTRACT Objective: This randomized study aimed to compare the clinical efficacy between the novel dual tracer composed of indocyanine green (ICG) and blue dye (BD) and the conventional dual tracer composed of radioisotope and BD for sentinel lymph node (SLN)mapping in patients with breast cancer.Methods: This study enrolled 471 clinically lymph node-negative patients with primary breast cancer. All patients underwent mastectomy, and those undergoing sentinel lymph node biopsy (SLNB) were randomized to receive blue dye plus radioisotope(RB group) or BD plus ICG (IB group). The detection performances on SLN identification rate, positive SLN counts, detection sensitivity, and false-negative rate were compared between the two groups.Results: In the IB group, 97% (194/200) of the patients who underwent the ICG and BD dual tracer injection showed fluorescentpositive lymphatic vessels within 2–5 min. The identification rate of SLNs was comparable between the IB group (99.0%, 198/200)and the RB group (99.6%, 270/271) (P = 0.79). No significant differences were observed in the identification rate of metastatic SLNs (22.5% vs. 22.9%, P > 0.05, RB group vs. IB group, the same below), positive SLN counts (3.72 ± 2.28 vs. 3.91 ± 2.13, P >0.05), positive metastatic SLN counts (0.38 ± 0.84 vs. 0.34 ± 0.78, P > 0.05), SLNB detection sensitivity (94.4% vs. 92.5%, P >0.05), or false-negative rate (5.6% vs. 7.5%, P > 0.05) between the two groups.Conclusions: ICG can be used as a promising alternative tracer for radioisotope in SLN mapping, and when it is combined with BD in lymphangiography, it offers comparable detection sensitivity compared to the conventional lymphatic mapping strategies that are widely used in clinical practice.
KEYWORDS breast cancer; indocyanine green; sentinel lymph node; biopsy; lymphography
Introduction
Breast cancer is the most frequently diagnosed cancer and the leading cause of cancer death among females worldwide1,2.Axillary lymph node status is the single most important prognostic indicator for the long-term outcome of patients with primary breast cancer, which is initially evaluated by axillary lymph node dissection (ALND)3. Since not all breast cancer patients should undergo this procedure, this aggressive technique has been replaced by sentinel lymph node biopsy (SLNB) for axillary staging in the late 20thcentury4,5. Since the early 1990s, blue dye (BD) and radioisotope have emerged as the most commonly used tracing agents to locate sentinel lymph node (SLN) in breast cancer6,7. The American Society of Clinical Oncology(ASCO) suggests that using the dual tracer of radioisotope and BD during SLNB could achieve a much higher SLN identification rate (> 90%) and a relatively low false-negative rate (< 5%–10%) than either tracer alone8. Moreover, the learning curve of using dual tracer instead of single tracer would not be significantly increased5,9,10.
Although intraoperative injection of radioisotope is both technically feasible and effective for SLN localization, this practice has not been widely adopted especially in developing countries, because it requires coordination with nuclear medicine personnel and/or special certifications for the surgeons11. Furthermore, injection of radioisotope the day before surgery has been found to offer some logistic advantages over same day injection, because same-day injection requires considerable coordination between the operating room and nuclear medicine personnel, which would profoundly affect the timing and efficiency of surgery12. Using a single dye as the sole tracer, on the other hand, results in low identification rate. Moreover, the success rate of SLN detection by the single dye method highly depends on the surgeon’s skills, and preoperative mapping of the SLN using this method is not feasible13. Therefore,finding an alternative preoperative, convenient and environmentally-friendly tracing reagent with uncompromised detection sensitivity and accuracy compared to the conventional tracers is the utmost demand for the SLNB procedure.
To overcome these limitations, several new techniques have been developed to detect SLNs. Indocyanine green(ICG), a near-infrared fluorescent dye, has been firstly employed in lymphatic mapping in 2005 by Kitai et al.14. This dye allows surgeons to visualize subcutaneous lymphatic vessels in real-time during surgery. Moreover, due to its nonallergenic and non-radioactive properties, ICG is an attractive alternative tracing reagent instead of radioisotope15. It has been shown that ICG alone identifies 93%–100% of SLNs, which is superior to BD alone and is comparable to radioisotope alone16,17. Our recent study also confirmed a comparable efficacy between ICG and radioisotope in SLN detection. However, compared to radioisotope, ICG has been shown to improve the identification rate of metastatic SLNs18.
Although ICG showed a favorable identification performance in SLN mapping, it still requires more extensive validation in terms of its efficacy, bio-safety, and side effects in large-scale clinical studies. Therefore, the efficacy between the ICG/BD combination (IB group) and the conventional radioisotope/BD combination (RB group) was thoroughly compared in SLN mapping in this prospective randomized study.
Patients and methods
Patients
Primary breast cancer patients with radiologically suspicious lymph nodes, pregnancy, inflammatory breast cancer, distant metastatic tumor, previous axillary surgery, or hypersensitivity to ICG were excluded from the study according to the 2014 ASCO Guideline Recommendations for Sentinel Lymph Node Biopsy in Early-stage Breast Cancer8and the 2013 Chinese Anti-Cancer Association(CACA) Guidelines and Standard Operating Procedures for Breast Cancer Diagnosis and Treatment19. Based on the exclusion criteria, between March 2015 and May 2017, in the Department of Breast Surgery of Southwest Hospital, Third Military Medical University, a total of 471 patients who were clinically negative for axillary lymph node were enrolled. All patients underwent mastectomy, while, for the SLNB, they were randomized to receive BD plus radioisotope or BD plus ICG. The clinical and pathological characteristics of the two groups were matched and are shown in Table 1. This present study was approved by the Ethical Committee of Southwest Hospital, Third Military Medical University. The study was approved by the Ethical Committee of Southwest Hospital,Third Military Medical University (Army Medical University). All enrolled patients signed an informed consent for study participation.
Reagents and equipment
BD (methylene blue dye, Jumpcan Pharmaceutical Group Co, Ltd, Taixing, China) was diluted to the final concentration of 1%, and ICG (Dandong Pharmaceutical,Jilin, China) was prepared at the final concentration of 1.25%.99Tcm-Dx (3.7 × 107Bq, Shihong Pharmaceutical,Beijing, China) was used as the radiotracer in the present study. The fluorescent vascular imaging system (MDM-I,Mingde, Langfang, China) and Neo2000 Gamma Detection System (Neoprobe Corporation, OH, USA) were used intraoperatively to detect the fluorescent signal of ICG and the radioisotope signal, respectively.
Procedure
Patients in the RB group were administered 1 mL of99Tcm-Dxat via subdermal injection in the disinfected periareolar region 4–12 h prior to surgery. Ten minutes before surgery, 1 ml of 1% BD was injected in the same region. All radioisotope-positive spots were properly labeled before a routine incision in the axilla was performed to expose all SLNs. Under the guidance of a gamma probe, radioisotopepositive SLNs were dissected from the lymphatic tissue and the axilla. All excised SLNs were further confirmed for the radioisotope-positive signal.
For the IB group, 1 mL of 1% BD was subdermally injected into the disinfected periareolar region 10 min before surgery.Subsequently, 1 mL of 1.25% ICG was injected intradermally into two to four spots at the same periareolar region followed by another 5-min massage. ICG fluorescence was detected by a portable fluorescent detector, and the lymphatic vessel was detected under fluorescence navigation and visualized on a monitor in real-time. The fluorescent signal was traced from the injection site (i.e., the periareolar region) to the axilla (or to the intramammary region in some cases). An incision was made at the position where the fluorescent signal disappeared, and anatomically this incision region was about 1 cm–3 cm distal to the axilla20and was the favorable accumulation site for SLNs (Figure 1). Fluorescent-positive lymph nodes were successfully detected after the skin and subdermal fat were incised. ALND was only conducted on patients with SLNs emitting fluorescent signals under the detector. The excised SLNs were double-checked under the detector to see if they were fluorescent positive.
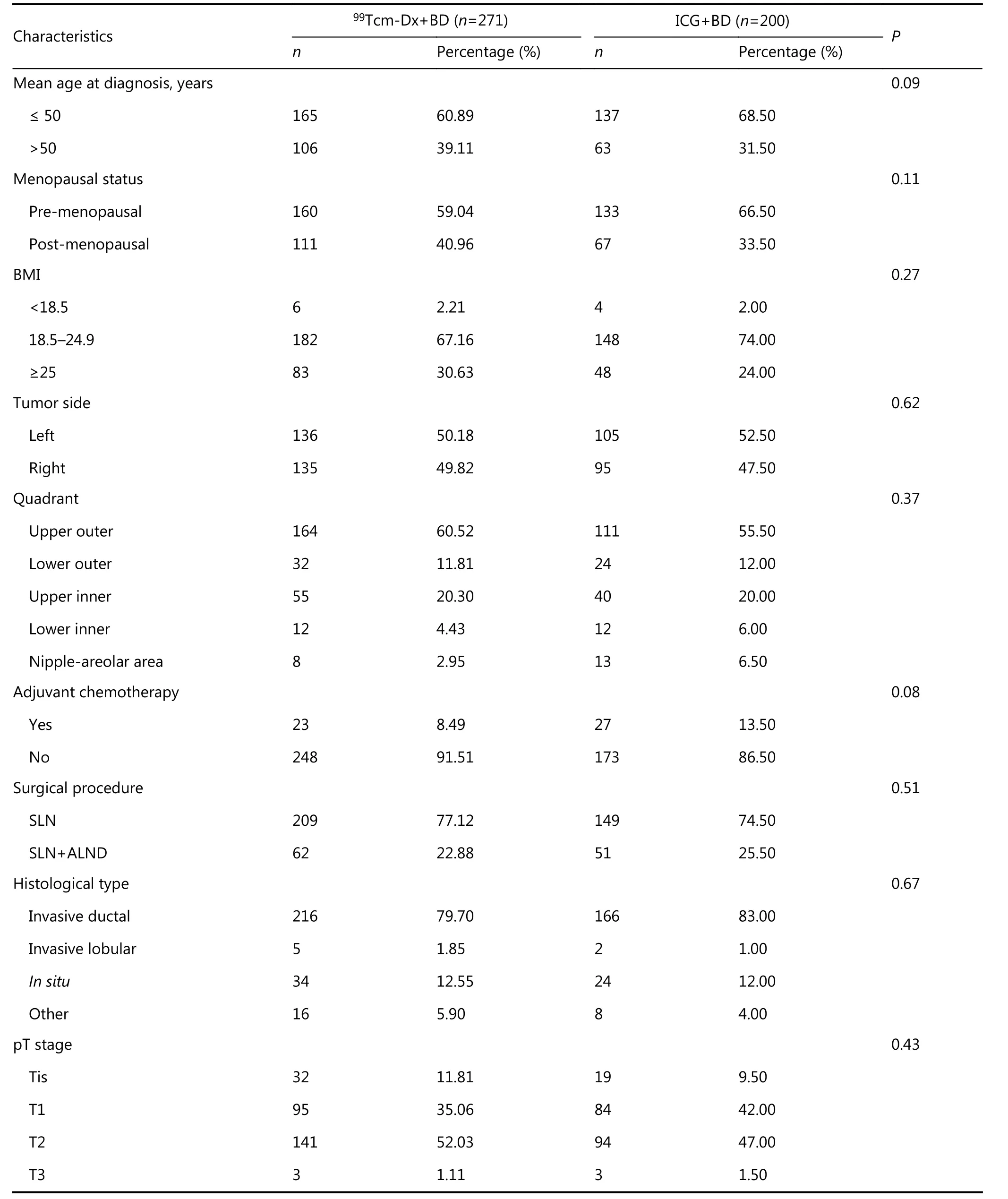
Table 1 Patient demographics and tumor characteristics
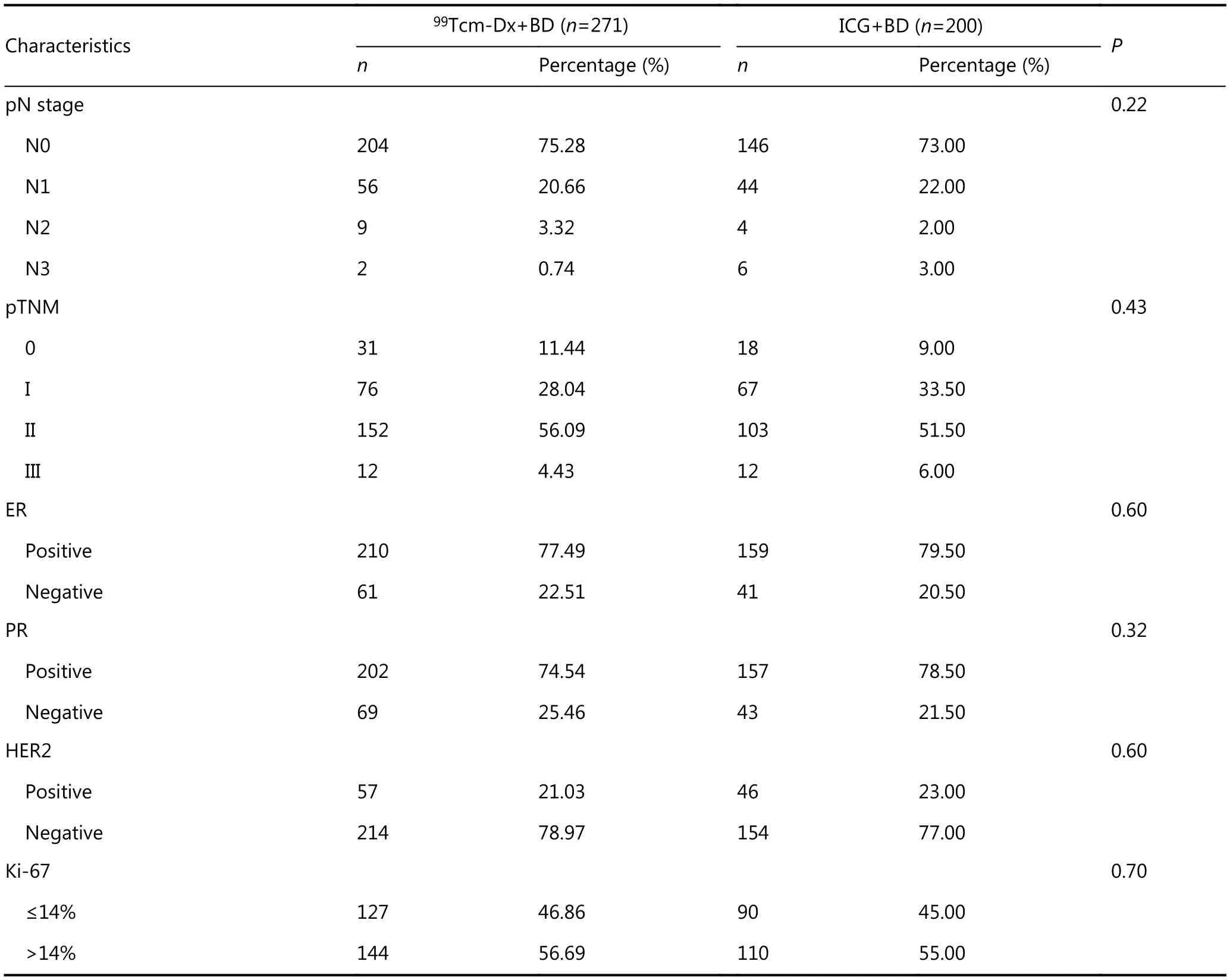
Continued
For both groups, BD-positive lymphatic vessels were localized under direct visualization, and BD-positive lymph nodes were further dissected. Finally, any anatomical abnormal (enlarged and/or infused) lymph nodes were dissected as well. Patients negative for SLN with either lymphatic mapping strategy were ruled out from the ALND procedure19.
Pathological examination and postoperative treatment
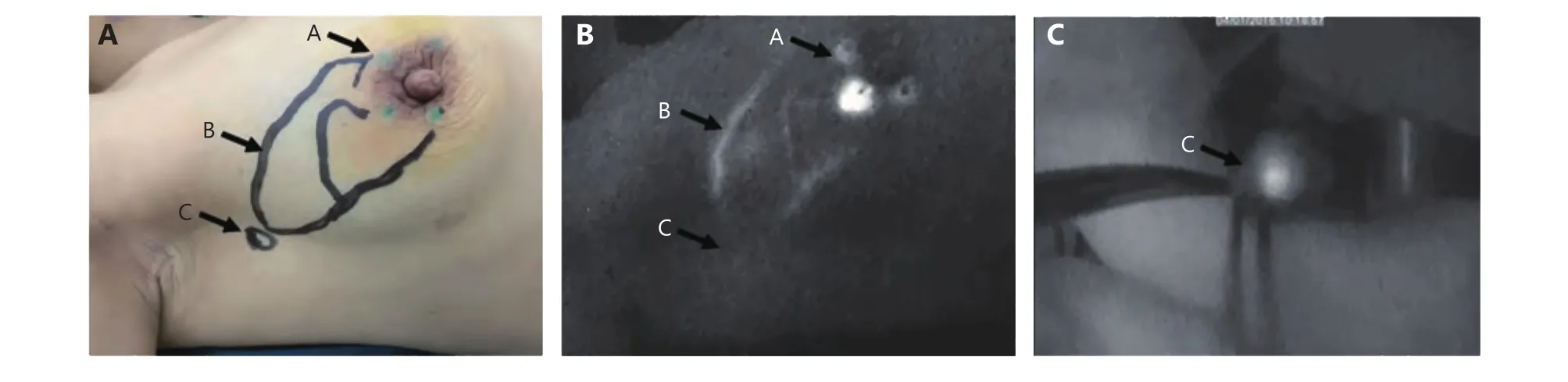
Figure 1 Indocyanine green revealed clear lymphatic pathway and lymph nodes under the fluorescent detector. (A) Injection site for indocyanine green. (B) A segment of fluorescent-positive lymphatic vessel. (C) An indocyanine green-positive sentinel lymph node.
All intraoperative SLN biopsies and removed nodes from both groups were submitted to the Pathology Department for cryosectioning and histological examination as previously reported21. Tumors that expressed estrogen receptor or progesterone receptor in at least 1% of the cells were considered ER- or PR-positive, tumors respectively. Human epidermal growth factor receptor 2 (HER2)-positive tumors were identified as showing increased expression levels of HER2 proteins, detected with immunohistochemistry,fluorescence in situ hybridization (FISH) or chromogenic in situ hybridization (CISH) methods. Ki-67 is an indicator of cell proliferation, and proliferation-positive tumors were those demonstrating more than 14% of Ki-67+cells in the tissues.
Based on the pathological results, patient-oriented intervention plans (i.e., chemotherapy, radiotherapy,endocrine therapy, or targeted therapy) were designed for each enrolled patient.
Follow-up
After the SLNB procedure, all patients were required to respond to the 24-month follow-up inquiries conducted by the researchers every six months either by visiting the doctors in person or by answering questions via telephone conversations. Parameters such as regional/systemic allergic reaction or anaphylaxis, infection at the injection site, distant metastasis, and upper limb lymphedema, in response to any of the tracer used in the study, were included in the followup. No drop-out was identified in either group.
Statistical analysis
For each modality, the SLN identification rate was calculated on the basis of the number of successful mappings divided by the total number of mappings performed. The metastatic SLN identification rate was calculated on the basis of the number of observed metastatic SLN divided by the total number of mapping cased performed. SLNB sensitivity was calculated on the basis of the number of patients with metastatic SLN detected by tracer materials divided by the total number of patients with metastatic SLN. The false negative rate was calculated on the basis of the number of patients negative for metastatic SLN mapped by tracer materials divided by the total number of patients with metastatic SLN. According to the 2014 ASCO Guidelines,patients who tested negative for SLN were excluded from the ALND procedure; therefore, we were unable to analyze the true-negative rate, positive predictive value, and negative predictive value for SLN.
Statistical analyses were performed using the IBM SPSS software (Version 19). The chi-square test was used to compare all parameters between the two groups. Average values are presented as mean ± SD. Statistical significance was recognized at P < 0.05.
Results
Demographics and tumor characteristics
The demographics and tumor characteristics of all enrolled patients are listed in table 1. Parameters such as average age,body mass index (BMI), tumor size and location, and staging were comparable between the two groups.
Indocyanine green acts as a convenient fluorescent-based lymphatic tracer for SLN identification
In this study, the fluorescent signal was detectable within 2–5 min after ICG injection at the periareolar region(Figure 1). Moreover, fluorescent-positive lymphatic vessels and SLNs showed strong signals under the fluorescent detector and were monitored on-screen in real-time.Although there were six cases with no visible fluorescent flow under the skin initially, fluorescent-positive signals in all of these individuals were detectable after a routine incision to expose the lymph nodes.
Indocyanine green shows a comparable nodal identification performance to the radioisotope 99Tcm-Dx when used in conjunction with blue dye
Comparison of the SLN detection performances between the control dual tracer (99Tcm-Dx+BD) and the experimental dual tracer (ICG+BD) showed comparable efficacy between ICG and radioisotope99Tcm-Dx. No statistical differences were observed in any examined parameters (i.e., SLN identification rate, SLN counts, metastatic SLN rate,metastatic SLN counts, detection sensitivity, or false-negative rate) between the two groups (Table 2).
Indocyanine green injection showed no allergic or side effects in patients during a 24-month follow-up period
During the 24-month follow-up, no side effects such as regional or systemic allergy or anaphylaxis, wound/injection site infection, upper limb lymphedema, or SLN local recurrence/metastasis were observed in either group after the SLNB procedure, indicating that ICG can be safely used as an allergic-free tracer in lymphatic mapping.
Discussion
In the current randomized study, clinical efficacy was compared between ICG + BD and radioisotope + BD for SLN mapping in breast cancer patients. No significant differences in the identification rate of SLNs, identification rate of metastatic SLNs, positive SLN counts, positive metastatic SLN counts, SLNB detection sensitivity, or falsenegative rate were detected between the two groups.Moreover, side effects were not detectable in either group during the 24-month follow-up. To the best of our knowledge, this is the first prospective controlled clinical study comparing the clinical value between ICG + BD and radioisotope + BD in SLN identification. We showed that ICG + BD could offer comparable performance to the conventional lymphatic mapping strategy, and therefore ICG can be used as a promising alternative tracer instead of radioisotope in SLN mapping.
The most commonly used tracing reagents for lymphatic mapping are BD and radioisotope. It has also been reported that BD could cause skin reactions, including intense erythema, superficial ulceration, and necrotic lesions22, and is also less false-negative intolerant than radioisotope during the SLNB procedure. However, radioisotope shows some inherent limitations. It has been reported to cause moderate and severe pain at the site of injection in many patients23.Moreover, the suboptimal spatial resolution of the detecting system and the lack of anatomic landmarks showing on the monitor hinder the accuracy of lymph node localization and numbers assessed even by experienced surgeons. All the above mentioned factors impede the wide application of radiotracer in clinical practice especially in developing countries such as China. Therefore, it is imperative to find a radioactive-free tracing reagent, which can be used in conjunction with BD as a dual tracer in lymphatic mapping to improve SLN identification sensitivity and additionally reduce the false-negative rate.
Since its first reported application in SLN identification in 2005, ICG, as a non-allergenic and non-radioactive fluorescent dye, has been increasingly used as a tracer for lymphatic mapping during the SLNB procedure in a variety of solid tumors24-26. Various studies in the setting of uterine malignancies have documented that the rate of detection for ICG is higher than that for blue dyes, Tc-99m, or a combination of blue dyes and Tc-99m27-29. However, in the breast cancer setting, ICG has not gained an equivalentclinical focus yet. The major limitation that hampered the clinical application of ICG for lymphatic mapping for breast cancer was the need for a portable, intraoperative imaging system to allow visualization of fluorescent subjects, which is not an issue anymore. According to a recent comprehensive systematic review16, using ICG as the tracing reagent can achieve an SLNB identification rate between 93.1% and 100%. In the fixed-effects model, ICG was significantly better than BD in terms of improving SLN identification sensitivity(OR = 18.37, 95% CI: 8.63–39.10). In contrast, no detectable difference in SLNB identification visualized by ICG and radiocolloid was observed in the random-effects model(OR = 0.81, 95% CI: 0.03–23.29). A recent meta-analysis conducted by Sugie et al.17showed that ICG was more sensitive than radiotracer in the fixed effects model (OR =1.87, 95% CI: 1.00–3.49). Other studies reported an identification rate of SLNs > 95% when using ICG and BD as a dual tracer30.
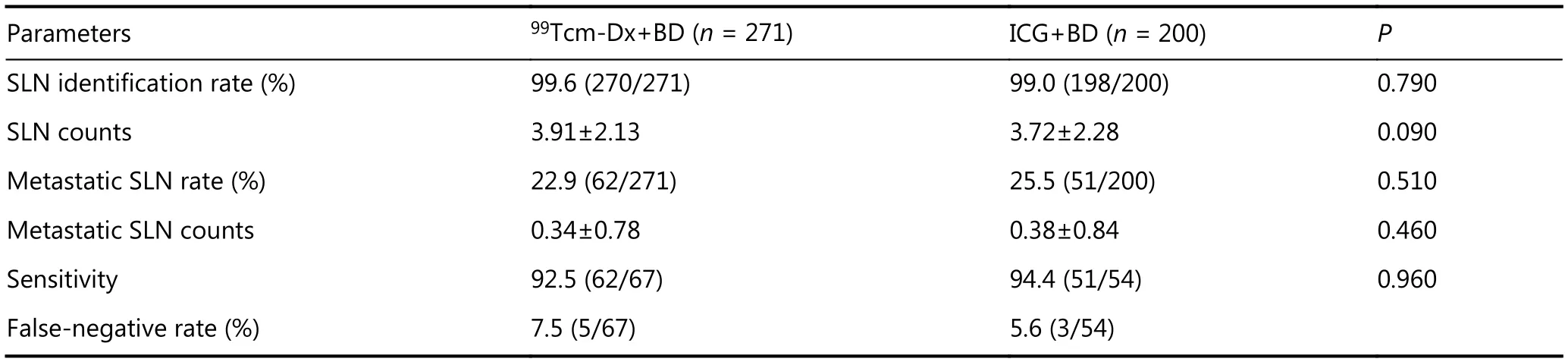
Table 2 Efficacy of indocyanine green vs. radioisotope + blue dye for sentinel lymph node mapping in breast cancer patients
Since studies regarding a comprehensive comparison of SLN identification performance between ICG + BD vs.radioisotope + BD are largely lacking, it is still controversial whether ICG can be used as a substitute for radiotracer in SLN detection16,31. Therefore, by taking advantage of having access to a large sample size of early-stage breast cancer patients in our hospital, this single-center prospective randomized study was designed to address this controversy.In the present study, ICG has been shown to rapidly emit a fluorescent signal in lymphatic vessels and SLNs after injection. A portable fluorescent detector provided the surgeon a clear subcutaneous lymphatic vessel fluorescent image on the monitor in real-time. Therefore, by injecting ICG in 200 patients, we achieved a 97% SLN identification rate, while when the SLN was exposed by axillary incision, we achieved a 99% SLN detection rate. It has been reported that BMI is significantly correlated with signal-negative lymphatic vessels32. Therefore, the injection depth and the thickness of adipose tissue might be the main factors that hindered the detection sensitivity of ICG. When the distance between the lymphatic vessel and fluorescent detector was larger than the normal range, detection is below limit. However, lymphatic vessel visualization was not necessarily correlated with SLN identification rate because in the present study, no fluorescent signal was detected under the skin of 6 patients,while when an incision was made in the axilla, the fluorescent-positive SLNs could be detected. Therefore, the present study suggests that ICG offers an acceptable efficacy in lymphatic vessel visualization and SLN identification,which together make it easier for the surgeons to locate the SLNs.
Interestingly, no statistical differences were observed in any of the examined parameters such as SLN identification rate and positive SLN counts between the radioisotope + BD group and the ICG + BD group, although it has been reported that ICG was superior to BD in detecting positive SLNs32. Moreover, the SLN identification rate of the traditional method (radioisotope + BD) was 96–97%according to international multi-center trials, such as the AMAROS33and ALMANAC trials34. In addition, the SLN identification rate of the novel technique (ICG + BD) in the current study was 99%, which was equivalent to the traditional method. It is generally accepted that the increased number of positive SLNs is inversely correlated with falsenegative rate. If only 1–2 SLNs were excised, the falsenegative rate would increase to 10%–17.7%. In contrast,when more than 3 SLNs were excised, the accompanied falsenegative rate could drop to 7%9. In the present study, the number of positive SLNs were all above 3; therefore, it was unsurprising that a low false-negative rate was achieved in both groups (5.6% in the RB group vs. 7.5% in the IB group).Since there were no differences in geographical parameters and tumor characteristics (potential confounders), such as age, BMI, tumor size and location, staging between control and experimental groups in the present study, it is safe to conclude that ICG could be used as an alternative tracer for radiotracer in SLN mapping in conjunction with BD.Moreover, given that no adverse effects were observed in patients receiving the ICG + BD dual tracer after a 24-month follow-up evaluation and ICG showed a better quality of care than radioisotope received by the patients35, it would be feasible to use ICG as a biologically and clinically safe tracing reagent for the SLNB procedure36,37.
Although ICG has been proved superior to BD in SLN identification16, ICG is preferred to be used in conjunction with BD for SLN mapping because of the following reasons.In the clinical practice, BD can serve as a complementary tracer for ICG, when the ICG fluorescent positive lymphatic vessel was cut accidentally while searching for SLNs. The fluorescent contamination at the surgical area caused by ICG leakage into the axillary adipose tissue could make it impossible to distinguish between the fluorescent-positive SLNs and the fluorescent-positive adipose tissue. In contrast,BD stained lymphatic vessels and lymph nodes can be easily detected by surgeons. Therefore, the SLN identification accuracy would not be compromised even when fluorescent contamination occurs when the dual tracer is used in the SLNB procedure.
Conclusions
The present study suggests that the dual tracer composed of ICG and BD could be used as a promising alternative tool for the gold standard combination of radioisotope and BD in SLN mapping. Considering that ICG is non-radioactive and that it is a fluorescent dye visible in real-time with high clinical performance, bio-safety as well as subjective feeling of patients, it shows great potential in the SLNB procedure.Large-scale randomized controlled clinical trials are warranted to further verify the current findings.
Acknowledgements
This work was supported by grants from the Clinical Research Founding of Southwest Hospital (Grant No.SWH2016BZGFKJ-30), Technological Innovation for Intelligent Medicine of Southwest Hospital (Grant No.SWH2016ZDCX4403), and Talents Training Program of Third Military Medical University (Grant No. 2017MPRC-18). We would like to extend our sincere gratitude and appreciation to Ying Zhang from University of San Francisco,San Francisco, CA, USA.
Conflict of interest statement
No potential conflicts of interest are disclosed.
 Cancer Biology & Medicine2018年4期
Cancer Biology & Medicine2018年4期
- Cancer Biology & Medicine的其它文章
- 2017 Chinese expert consensus on the clinical application of serum marker for thyroid cancer
- Multidisciplinary team for the diagnosis and treatment of 2 cases of primary intestinal yolk sac tumor
- Prognostic factors of refractory NSCLC patients receiving anlotinib hydrochloride as the third- or further-line treatment
- PD-L1 expression and its effect on clinical outcomes of EGFR-mutant NSCLC patients treated with EGFR-TKIs
- Five-CpG-based prognostic signature for predicting survival in hepatocellular carcinoma patients
- A new tumor-associated antigen prognostic scoring system for spontaneous ruptured hepatocellular carcinoma after partial hepatectomy