
Guidelines for the diagnosis and treatment of follicular lymphoma in China
2013-09-26 06:01:06HematologyBranchofChineseMedicalAssociationChina
Cancer Biology & Medicine 2013年1期
Hematology Branch of Chinese Medical Association, China
Follicular lymphoma (FL) is a common subtype of B-cell lymphoma.Based on the updated National Comprehensive Cancer Network guidelines and related medical data, the authors formulated the FL guidelines for China by combining the diagnostic level and current situation of lymphoma.
Definition
Follicular lymphoma (FL) is a common type of non-Hodgkin’s lymphoma (NHL), accounting for 22% to 35% of NHL in western countries.The proportion in China, 8.1%to 23.5%, is less than that in western countries, although its incidence in China has increased with time.Compared with foreign countries, the age of onset is younger in China, and in terms of geographical distribution, the incidences in coastal regions and economically developed areas are higher1-3.
FL is from germinal-center B-cells, and is manifested morphologically as a tumor retaining follicular growth.FL comprises a group of malignant lymphoproliferative diseases including follicular center cells (small cleaved cells)and follicular center matricytes (large non-cleaved cells).Under microscopy, FL sometimes appears to be associated with diffused components.Based on different follicular components and their proportions, FL can be divided into the following (1) follicle-dominant type (proportion of follicles >75%); (2) follicle and diffuse mixed type (follicles accounting for 25% to 75%); and (3) focal follicle (proportion of follicles <25%)4,5.
Diagnosis, staging, prognosis, and differential diagnosis
Diagnosis
The diagnosis of FL is mainly based on histopathological examination, including immunohistochemical and morphological examination, although it can also be based on the results of flow cytometric and cytogenetic analyses, if necessary.
According to the lymphoma classification of the World Health Organization, FL can be further divided into stages 1 to 3.In Stage 1, 0 to 5 matricytes are present per high-power field;in Stage 2, 6 to 15 matricytes are present per high-power field;and in Stage 3, the number of matricytes per high-power field >15, among which the remaining few centrocytes are referred to as Class 3A, while Class 3B is characterized by infiltrated flaky central matricytes and the absence of centrocytes.The clinical manifestation of FL in Class 1-2 and 3A is inertia, and that in Class 3B is manifested by invasion similar to diffuse large B-cell lymphoma (DLBCL).Currently,FL in Class 1-2 is based on the treatment principles of indolent lymphoma.FL in Classes 3A and 3B is treated with the treatment principles of DLBCL, and the clinical effects are similar.After a few years of treatment, the diagnosis of several FL patients changes to invasive lymphoma, mainly invasive DLBCL with poor prognosis6,7.
FL has a characteristic immunophenotype and B-cell markers are expressed in cell surface.Immunohistochemical detection generally uses the following group of indices: CD20,CD3, CD5, CD10, Bcl-6, Bcl-2, CD21, CD23, and cyclinD1.Ki-67 is typically recommended for assessment.The typical immunohistochemical markers are CD20+, CD23+/-, CD10+,CD43-, Bcl-2+, Bcl-6+, CD5-, and CCND1-, while Bcl-2- or CD10- also appear in several cases.Molecular genetic testing can help identify bcl-2 rearrangement, while cytogenetics or fluorescence in situ hybridization inspection t (14;18) or t(8;14) can facilitate diagnosis.
Inspection, staging, and prognosis of FL
The diagnostic test of FL is similar to other indolent lymphoma inspections.The necessary steps include the following: general physical examination, particularly to check if super ficial lymph node, liver, and spleen are enlarged; laboratory examination,including complete blood cell inspection, blood biochemical inspection, as well as serum lactate dehydrogenase (LDH)level, hepatitis B and C, and HIV-related detection; and imaging examinations via enhanced computed tomography(CT) detection of neck, chest, abdomen, and pelvic cavity and via bilateral or unilateral bone marrow biopsy plus smear examination, which are recommended to be performed routinely.The sample for bone marrow biopsy should be at least larger than 1.6 cm.Using positron emission tomography (PET)/CT is helpful in detecting some non-palpable lesions, but its clinical value is lower than those found in DLBCL and Hodgkin's lymphoma subtype.In addition, PET/CT can help diagnose FL transformation.
To predict FL prognosis, the standard of FL International Prognosis Index (FLIPI) is as follows: for FLIPI-1, age ≥60,Ann Arbor staging includes stages III to IV, hemoglobin(HBG) <120 g/L, serum LDH >upper limit of normal range,and involved lymph nodes ≥5.Each indicator refers to a score of 1.According to the scores, FL patients can be divided into three risk groups, namely, low risk, intermediate risk,and high risk.In recent years, with the increasingly common use of IDEC-C2B8 (rituximab) for treating FL, the new clinical prognostic scoring system, FLIPI-2, is considered an improved version of FLIPI-1.FLIPI-2 includes the following factors: β2-microglobulin > upper limit of normal range, maximal lymph node diameter>6 cm, bone marrow being violated, HGB <120 g/L, and age >60 (Table 1).
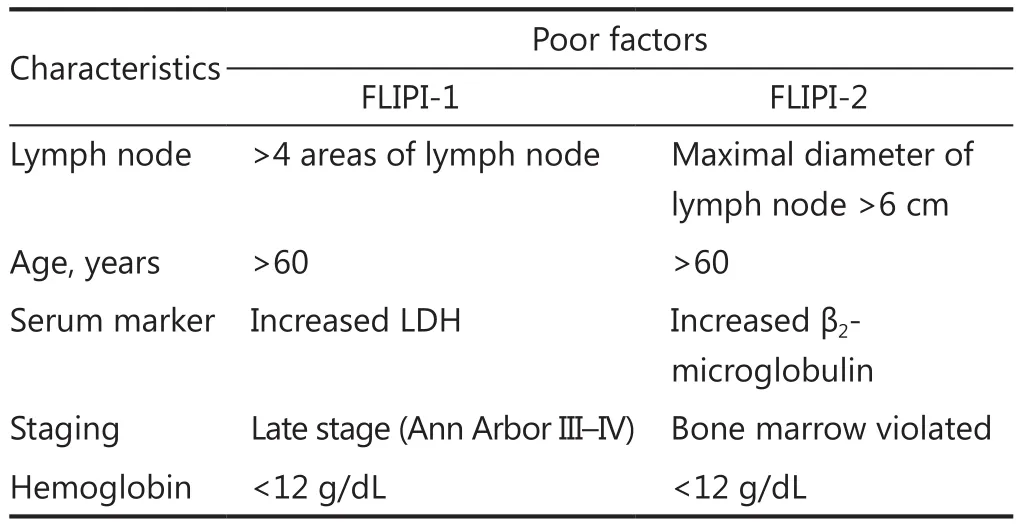
Table 1 FLIPI-1 and FLIPI-2
Treatment of FL
Treatment indicators
Localized radiation therapy is mainly adopted for FL patients in Stages I and II.The disease-free survival is extended for most patients.Therefore, radiation therapy or radiation therapy associated with general immunochemotherapy should be adopted as soon as possible.
Currently, FL patients in Stage II with abdominal mass and Stages III to cannot be cured with the available treatment methods.Most patients have slow disease progression and can maintain better quality of life, even if treatment is not for a long time.Thus, a patient can be treated if one of the following treatment indicators is exhibited (Table 2).
The following items should be detected before treatment: (1)disease history; (2) physical examination aimed at identifying possible areas of lymph node accumulation and the sizes of the cerebral arterial circle and liver and spleen; (3) physical condition; (4) B symptoms; (5) complete blood count and biochemical routine; (6) CT scans of the neck, chest, abdomen,and pelvis; (7) hepatitis B virus detection; (8) bone marrow biopsy and smear; (9) routine electrocardiogram.
Ultrasonic cardiogram of the left ventricular ejection fraction, PET/CT, β2-microglobulin, uric acid, serum protein electrophoresis, and/or quantitative immunoglobulins and Hepatitis C-related examination can also be performed, if necessary.
Front-line treatment options of FL patients in Stages I to II
FL patients in level 3 should be treated based on DLBCL treatment strategy.Enough clinical evidence has shown that involved field radiation therapy (IFRT) is an ideal treatment option for FL patients in stages I to II of levels 1 and 2.Improved long-term survival rate can be achieved by simple radiation treatment, with a radiation dose of 30 Gy to 36 Gy.Although the efficacy of general immunochemotherapy associated with the radiation treatment for FL patients in Stages I to II has yet to be fully explored, several reports have pointed out that such treatment could improve survival.Watchful monitoring is recommended if the risk of adverse reactions of FL patients for IFRT is estimated to be greater than the probability of clinical benefits.Front-line-associated immunochemotherapy may be recommended for patients in Stages I to II with high tumor burden or patients in FLIPI intermediate and high risk (>1 score)8.
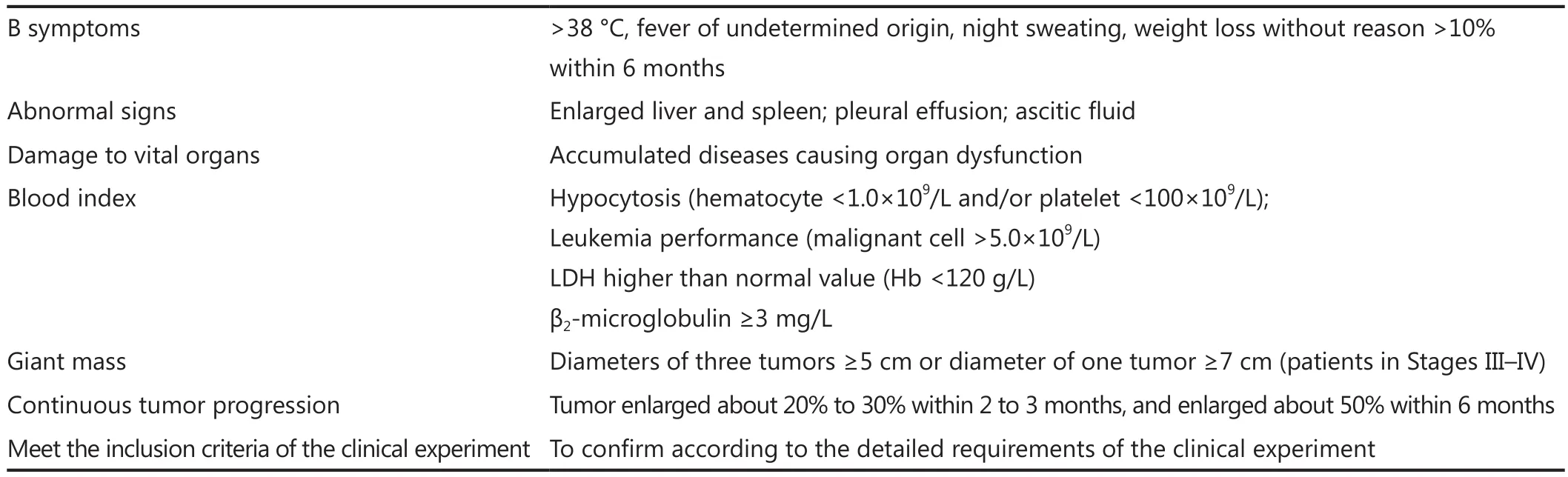
Table 2 Treatment indicators
Front-line treatment of FL patients in Stages III to IV
Compared with FL in Stages I to II, FL in Stages III to IV is generally considered an incurable disease.The watchful monitoring strategy can be adopted if patients have no treatment indicators (Table 2).For FL patients in Stages III to IV with treatment indicators, the treatment options are more current, and the general principle is to choose a highly individual treatment program based on age, general physical conditions, complications,and treatment goal.
Immunochemistry is currently the most commonly selected treatment mode at home and abroad.The treatment program with 8 courses of rituximab associated with chemotherapy has become the preferred standard program at home and abroad for the initial treatment of FL patients.Regardless of which treatment is chosen (i.e., CHOP, CVP program, or fludarabine associated with rituximab), all treatment methods have been shown to improve recent and long-term effects significantly, including overall survival.Therefore, routine dose of associated chemotherapy plus rituximab is suggested for relatively young patients with better constitution9,10.
Meanwhile, researchers have still not reached a consensus on the optimal front-line treatment program for late-stage FL patients,either by chemotherapy associated with rituximab or single-agent rituximab.Nevertheless, the result of a recent FOLL05 experiment shows that R-CHOP program is better than R-CVP or R-FM program based on risks and bene fits.Several studies have shown that fludarabine has toxicity on bone marrow stem cells and is related to secondary tumor.Therefore, premature use should be avoided, particularly for patients with autologous hematopoietic stem cell transplantation (ASCT).
For weak and old patients who are unable to endure combination chemotherapy, single-agent rituximab, singleagent chemotherapy, or rituximab associated with single-agent chemotherapy can be selected for front-line treatment.In addition,supportive treatment should be enhanced.
The treatment rule of relapsed FL patients
Regardless of the type of induced immunochemotherapy adopted, relapse can occur after a period of disease remission.As of this writing, the standard treatments for relapsed, intractable FL patients have yet to be unified.The option for salvage therapy depends on the curative effects of previous programs, release time, age of patients, physical conditions, pathologic types at relapse, and treatment goal.For the relapsed patients without transformation and with long-term remission after front-line treatment, the original program or other front-line programs can be used.For the early relapsed patients (<12 months), noncross drug-resistant program (e.g.fludarabine, can be used as salvage program if relapse occurs after CHOP treatment) can be selected and applied.The effective rate of rituximab for treating relapsed FL is around 45%, whereas the rate for CR is 6%.Rituximab can also increase the effect of salvage chemotherapy.The salvage chemotherapy options include CHOP, fludarabinebased program, CVP, and radioimmunotherapy.New drugs and new combined programs can also be considered.Thus, it is recommended that ASCT be adopted in the treatment of relapsed young patients9,10.
Maintenance treatment of FL
FL patients with a long disease history and slow progress are more sensitive to various treatments.Thus, maintenance treatment is suitable for these patients after remission induction.Numerous clinical studies and meta-analysis results have proven that, for FL patients after front-line treatment or one more remission induction of relapse, the maintenance treatment via single-agent rituximab improves long-term survival11-14.Therefore, the recommended treatment for patients being initially treated or relapsed patients after induction chemotherapy and complete remission (CR) or partial remission (PR) is one maintenance treatment by single-agent rituximab every 2 to 3 months, for a total of 2 years.However, the probability of infection can increase after maintenance treatment.Close follow-up and observation should be given to hepatitis B patients15.
Treatment of conversion FL lymphoma
Around 20% to 70% of FL that occur in patients can be clinically transformed into other more invasive lymphomas.The most common of these invasive lymphomas is DLBCL, which has an annual incidence rate of 2% to 3% and has continued to increase for at least 15 years.After this period, the transformation risk decreases gradually, after which the transformation is no longer affected regardless of whether or not FL patients have ever been treated.Most patients, after undergoing transformation,have poor prognosis, with a median survival time of 10 to 18 months.Uneven values in FDG-PET scanning and increasing standardized uptake value can show the transformation, which should be verified by biopsy.
Currently, no standard therapeutic measure exists for transformative FL; thus, the therapeutic measure of transformed invasive lymphoma can be adopted.The patients treated by mild chemotherapy or those who have not recieved chemotherapy can choose anthracycline-based combined chemotherapy ± radiation treatment or chemotherapy ± rituximab, in order to achieve better outcome.If patients have been previously treated strongly by numerous kinds of chemotherapy programs, IFRT or other chemotherapy programs can be considered.These patients with poor prognosis are recommended to participate in clinical trials.If patients are sensitive to chemotherapy, hematopoietic stem cell transplantation, particularly ASCT, should be considered for administration after they are eased again into treatment.Meanwhile, allogeneic hematopoietic stem cell transplantation(allo-HSCT) may be attempted in a small number of highly selected patients.
Hematopoietic stem cell transplantation
The therapeutic action of high-dose chemotherapy supported by ASCT on FL patients in Stages III to IV remains controversial.Various studies have shown that ASCT is not highly effective for patients being eased initially, and that autologous transplantation can extend the survival time of FL patients with sensitive relapse (1 to 4 relapses by preference).Therefore, FL patients in Stages III to IV who are still sensitive to chemotherapy after numerous relapses are encouraged to participate in such kind of clinical trial, especially if they are young or have good physical conditions with improved function of vital organs.With the continuous progress of allo-HSCT, myeloablative or non-myeloablative allo-HSCT have initially shown long-term survival benefits for several patients.However, the problem of high transplantation-related mortality rate still needs to be solved.Currently, allo-HSCT is only suitable for a small number of patients for research.
Treatment of untoward effects
Details are found in the relative treatment guidelines of DLBCL in China.
Criterion of therapeutic effects
Currently, the 1999 guidebook published by the International Working Group and the 2007 guidebook revised by the International Coordination Scheme are adopted as the criteria of the therapeutic effects of lymphoma.The criterion in the 1999 version is based on the reduced size of the swelled lymphadenopathy measured by CT, and the level of bone marrow being infiltrated con firmed by smear and biopsy.The therapeutic effects are divided into CR, uncertain complete remission (CRu), PR, steady (SD),and relapse or development (PD).FDG-PET/CT is added into the criterion in the 2007 version.PET/CT can determine if the residual mass is PR or CR; thus, the revised criterion cancelled CRu, and kept CR, PR, SD, and PD.Imaging review should be done at least 3 weeks after the end of chemotherapy.The detailed evaluation of therapeutic effects is shown in Tables 3 and 4.
Follow-up
Follow-up must be conducted every 2 to 3 months in the first year for patients in remission stage (CR or PR) after all treatment methods.Then, one follow-up every 3 months should be conducted in the second year, followed by one follow-up every 6 months.The follow-up sessions may also be scheduled according to clinical indications.Follow-up content covers repeat diagnostic test, imaging examination based on the clinical situations (i.e., depending on disease region and clinical feature), and physical examination.
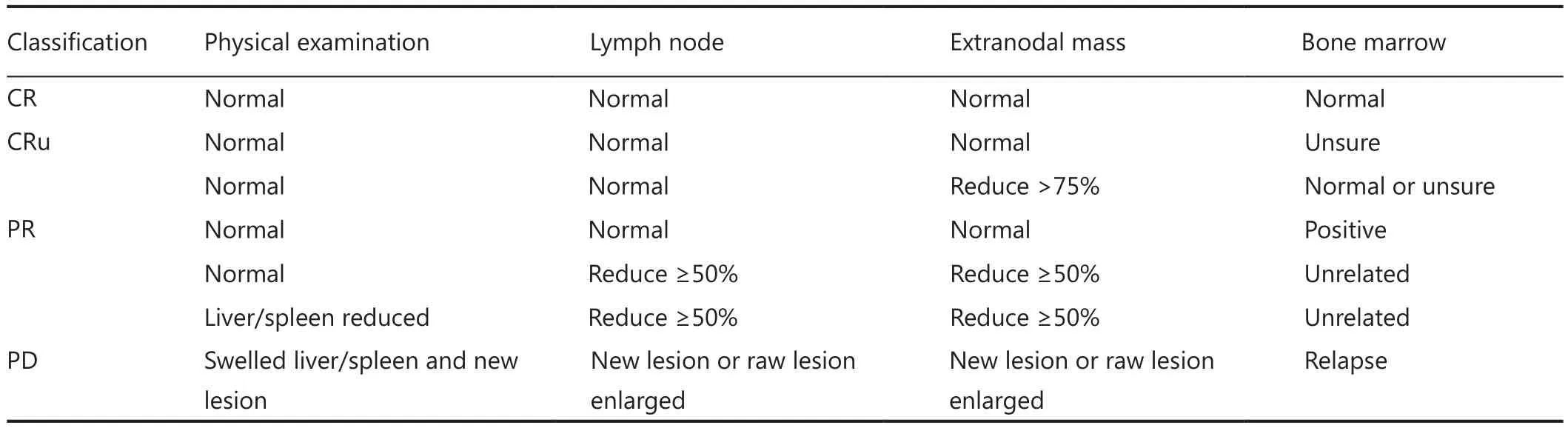
Table 3 Criteria of therapeutic effects (excluding PET)
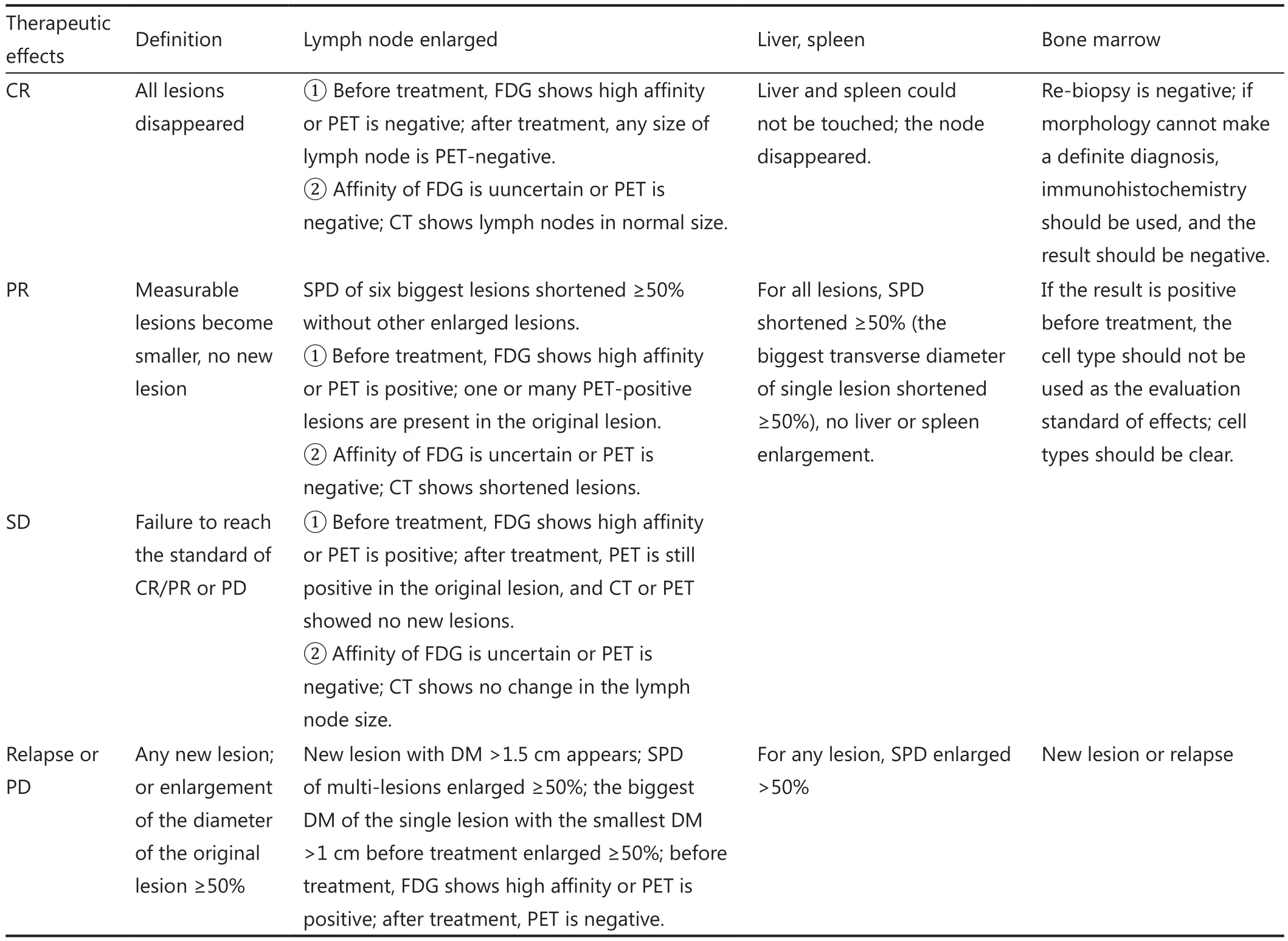
Table 4 Revised criteria of therapeutic effects (including PET)
Appendix: The main treatment programs of FL
Front-line treatment program
Single agent: Chlorambucil and/or single-agent rituximab.This program is suitable for old and weak patients.
R-CHOP: Rituximab is administered in the first day, repeated every 3 to 4 weeks, 8R-6CHOP.This program is one of the most common standard treatment programs for FL patients.For old patients with cardiac dysfunction, epidoxorubicin (epirubicin),pirarubicin, or liposomal doxorubicin can be used to replace conventional doxorubicin.
R-CVP: This program is also one of the most common standard treatment programs for FL patients.R-CVP is milder than R-CHOP, and is suitable for old patients with cardiac dysfunction.
R-F: Rituximab is administered in the first day, whereas fludarabine is given for 2 to 4 d, and then repeated every 28 d.Note: immunological suppression is more obvious, and patients can easily be infected.
Consolidation or maintenance treatment after front-line treatment: Rituximab is used for maintenance treatment after immunochemotherapy remission.The dosage of rituximab is 375 mg/m2, once every 2 to 3 months for a total of 2 years.Notes: patients in CR/CRu/PR after inductive treatment will be given maintenance treatment; low immunoglobulinemia can appear during maintenance treatment, and patients can recover on their own even if rituximab is not administered.
Second-line treatment program
If a longer non-treatment gap exists after front-line treatment, the original treatment program can be considered to be continuously used once relapse occurs.
R-FC: Rituximab is administered in the first day, whereas fludarabine and CTX are given for 2 d to 4 d, to be repeated every 28 d.Note: preventive Pneumocystis carinii pneumonia treatment should be considered.
R-F: Rituximab is administered in the first day, whereas fludarabine is given for 2 d to 4 d, to be repeated every 28 d.
The following DLBCL second-line program can be considered: ESHAP (etoposide + methylprednisolone+ cis-platinum + Ara-C) ±rituximab; GDP (gemcitabine+ dexamethasone + cis-platinum) ±rituximab; GemOX(gemcitabine + oxaliplatin) ±rituximab; ICE (ifosfamide+ carboplatin + etoposide) ±rituximab; single-agent Thalidomide; full oral PEPC program.Note: the highly individual dose adjustment and time arrangement should be selected according to the actual conditions of the patients.
Second-line maintenance treatment program
A dose of 375 mg/m2of rituximab is administered for 2 years,and repeated every 2 to 3 months.Notes: CR/PR patients undergo maintenance treatment after inductive treatment;prognosis is poor for patients with repeated relapse; thus, these patients are encouraged to participate in clinical research.
Acknowledgements
The following experts participated in the discussion of this guideline.Prof.Zhi-xiang Shen and Prof.Jun-min Li (Shanghai Jiao Tong University School of Medicine, Ruijin Hospital);Prof.Xiao-jun Huang and Prof.Qian Jiang (Peking University People’s Hospital); Prof.Jian-xiang Wang and Prof.Lu-gui Qiu(Institute of Hematology & Blood Diseases Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College);Prof.Jian-yong Li (The First Afflicted Hospital of Nanjing Medical University); Prof.Jun Ma (Harbin Tumor Institute of Hematology); Prof.Ti Shen and Prof.Yong-qiang Zhao (Peking Union Medical College Hosptial); Prof.De-pei Wu (The First Affiliated Hospital of Soochow University); Prof.Jie Jin (Then First Affiliated Hospital of Zhejiang University); Prof.Jian-min Wang (Shanghai Changhai Hosptial); Prof Ting Liu (Sichuan University West China Hospital); Prof.Jian-da Hu (Fujian Medical University Union Hosptial); Prof.Li Yu (Chinese PLA General Hospital); Prof.Juan Li (The First Affiliated Hospital of Sun Yat-sen Universtiy); Prof.Zhong-zhen Guan, Prof.Wenqi Jiang and Prof.Hui-qiang Huang (Yat-sen Universtiy Cancer Center); Prof.Yuan-kai Shi (Cancer Institute & Hosptial,Chinese Academy Medical Sciences); Prof.Jun Zhu (Beijing Cancer Hospital); Prof.Xiao-nan Hong (Shanghai Fudan University Cancer Hospital); Prof.Hua-qing Wang (Tianjin Medical University Cancer Institute & Hospital).
Conflict of interest statement
No potential conflicts of interest are disclosed.
1.Zhou LQ, Sun Y, Tan WY, Li T, Wang QL, Feng FY, et al.The clinical and pathological analysis for 1125 cases with non- Hodgkin’s lymphoma.Aizheng Jinzhan 2006;4:391-397 (in Chinese).
2.Cheng YX, Xu W, LI JY, Qian SX, Lu H, Wu HX, et al.Clinical analysis of 641 cases of non-Hodgkin’s lymphomas.Nanjing Yike Daxue Xuebao 2006;26:837-840 (in Chinese).
3.Xiao C, Su ZL, Wu QL, Gao HY, Clinical and pathological reassessment of 493 cases of non-Hodgkin’s lymphomas according to current WHO classi fication of lymphoid neoplasms.Zhonghua binglixue Zazhi 2005;34:22-27 (in Chinese).
4.Vitolo U, Ferreri AJ, Montoto S.Follicular lymphomas.Crit Rev Oncol Hematol.2008;66:248-261.
5.NCCN Clinical Practice Guidelines in Oncology.Version 1.2012.
6.Dreyling M, Ghielmini M, Marcus R, Salles G, Vitolo U, ESMO Guidelines Working Group.Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up.Ann Oncol 2010;21:181-183.
7.Solal-Céligny P, Roy P, Colombat P, White J, Armitage JO, Arranz-Saez R, et al.Follicular lymphoma international prognostic index.Blood 2004;104:1258-65.
8.Petersen PM, Gospodarowicz M, Tsang R, Pintilie M, Wells W,Hodgson D, et al.Long-term outcome in stage I and II follicular lymphoma following treatment with involved field radiation therapy alone.J Clin Oncol 2004;22:561.
9.Hiddemann W, Kneba M, Dreyling M, Schmitz N, Lengfelder E, Schmits R, et al.Frontline therapy with rituximab added to the combination of cyclophosphamide, doxorubicin, vincristine,and prednisone (CHOP) significantly improves the outcome for patients with advanced-stage follicular lymphoma compared with therapy with CHOP alone: results of a prospective randomized study of the German Low-Grade Lymphoma Study Group.Blood 2005;106:3725-3732.
10.Marcus R, Imrie K, Belch A, Cunningham D, Flores E, Catalano J, et al.CVP chemotherapy plus rituximab compared with CVP as first-line treatment for advanced follicular lymphoma.Blood 2005;105:1417-1423.
11.Hochster H, Weller E, Gascoyne RD, Habermann TM, Gordon LI, Ryan T, et al.Maintenance rituximab after cyclophosphamide,vincristine, and prednisone prolongs progression-free survival in advanced indolent lymphoma: results of the randomized phase III ECOG1496 Study.J Clin Oncol 2009;27:1607-1614.
12.van Oers MH, Klasa R, Marcus RE, Wolf M, Kimby E, Gascoyne RD, et al.Rituximab maintenance improves clinical outcome of relapsed/resistant follicular non-Hodgkin lymphoma in patients both with and without rituximab during induction: results of a prospective randomized phase 3 intergroup trial.Blood,2006;108:3295-3301.
13.van Oers MH, Van Glabbeke M, Giurgea L, Klasa R, Marcus RE,Wolf M, et al.Rituximab maintenance treatment of relapsed/resistant follicular non-Hodgkin’s lymphoma: long-term outcome of the EORTC 20981 phase III randomized intergroup study.J Clin Oncol 2010;28:2853-2858.
14.Salles G, Seymour JF, Offner F, López-Guillermo A, Belada D,Xerri L, Feugier P, et al.Rituximab maintenance for 2 years in patients with high tumour burden follicular lymphoma responding to rituximab plus chemotherapy (PRIMA): a phase 3, randomised controlled trial.Lancet 2011;377:42-51.
15.Huang YH, Lin HC, Lee SD.Management of chemotherapyinduced hepatitis B virus reactivation.J Chin Med Assoc 2012;75:359-362.
 Cancer Biology & Medicine2013年1期
Cancer Biology & Medicine2013年1期
- Cancer Biology & Medicine的其它文章
- Combined transfection of Bcl-2 siRNA and miR-15a oligonucleotides enhanced methotrexate-induced apoptosis in Raji cells
- Reduced-intensity conditioning allogeneic stem cell transplantation in malignant lymphoma: current status
- A novel t(3;12)(q21;p13) translocation in a patient with accelerated chronic myeloid leukemia after imatinib and nilotinib therapy
- Adenoid cystic carcinoma in the maxillary gingiva: a case report and immunohistochemical study
- Spontaneous pineal apoplexy in a pineal parenchymal tumor of intermediate differentiation
- Research development of the relationship between thymidine phosphorylase expression and colorectal carcinoma