
Drainage vs.non-drainage after cholecystectomy for acute cholecystitis:a retrospective study
2014-04-18 13:18:52MohmmeBwhWliElMksouSeeAlsreiiFhAlAmriHlAliAulRhmnNimeriAulRhmnAlAmriAelAssiriMohmmeAulAziz
Mohmme A Bwh,Wli M A El Mksou,?,See A Alsreii,Fh S Al Amri,Hl F Ali,Aul Rhmn Nimeri,Aul Rhmn M Al Amri,Ael A Assiri,Mohmme I Aul Aziz
aGeneral Surgery Department,Faculty of Medicine,King Khalid University,Abha 61421,Saudi Arabia;
bGeneral Surgery Department,Faculty of Medicine,Najran University,Najran,P.O.1988,Saudi Arabia;
cGeneral Surgery Department,Sheikh Khalifa Medical City,Abu Dhabi,P.O.51900,United Arab Emirates;
dGeneral Surgery,Abha Private Hospital,Abha 61431,Saudi Arabia.
Drainage vs.non-drainage after cholecystectomy for acute cholecystitis:a retrospective study
Mohammed A Bawahaba,Walid M Abd El Maksouda,?,Saeed A Alsareiib,Fahad S Al Amria,Hala F Alia,Abdul Rahman Nimeric,Abdul Rahman M Al Amrib,Adel A Assirib,Mohammed I Abdul Azizd
aGeneral Surgery Department,Faculty of Medicine,King Khalid University,Abha 61421,Saudi Arabia;
bGeneral Surgery Department,Faculty of Medicine,Najran University,Najran,P.O.1988,Saudi Arabia;
cGeneral Surgery Department,Sheikh Khalifa Medical City,Abu Dhabi,P.O.51900,United Arab Emirates;
dGeneral Surgery,Abha Private Hospital,Abha 61431,Saudi Arabia.
Many surgeons practice prophylactic drainage after cholecystectomy without reliable evidence.This study was conducted to answer the question whether to drain or not to drain after cholecystectomy for acute calculous cholecystitis.A retrospective review of all patients who had cholecystectomy for acute cholecystitis in Aseer Central Hospital,Abha,Saudi Arabia,was conducted from April 2010 to April 2012.Data were extracted from hospital case files.Preoperative data included clinical presentation,routine investigations and liver function tests.Operative data included excessive adhesions,bleeding,bile leak,and drain insertion.Complicated cases such as pericholecystic collections,mucocele and empyema were also reported.Patients who needed therapeutic drainage were excluded. Postoperative data included hospital stay,volume of drained fluid,time of drain removal,and drain site problems. The study included 103 patients allocated into two groups;group A(n=38)for patients with operative drain insertion and group B(n=65)for patients without drain insertion.The number of patients with preoperative diagnosis of acute non-complicated cholecystitis was significantly greater in group B(80%)than group A(36.8%)(P<0.001). Operative time was significantly longer in group A.All patients who were converted from laparoscopic to open cholecystectomy were in group A.Multivariate analysis revealed that hospital stay was significantly(P<0.001)longer in patients with preoperative complications.There was no added benefit for prophylactic drain insertion after cholecystectomy for acute calculous cholecystitis in non-complicated or in complicated cases.
acute cholecystitis,routine drainage,cholecystectomy,subhepatic collection
INTRODUCTION
Drainage of body cavities has been practiced in medicine for a long time[1].Historical reports of drainage of chest empyema and ascites go back to the Hippocratic era[2].However,abdominal drainage has always been a subject of controversy,practiced in confusion and subjected to local dogmas[3].A hundred years have passed during which operative surgery and supportive care techniques have progressed astonishingly;but what about drainage?Is the practice of drainage anyless controversial,more rational and less confusing today[4]?
Surgeons aim differently when using abdominal drainage,either for prophylaxis or therapy.For thera-peutic reasons,drainage is used for established infection,e.g.peri-appendicular abscess or diffuse fecal peritonitis,and to control a source of infection that cannot be controlled by other means by creating a‘‘controlled’’external fistula(i.e.,a leaking duodenal suture line)[5].Drains are also placed to provide a passage for established intra-abdominal collections such as ascites,blood,bile,chyle,and pancreatic or intestinal juice.These collections might become potentially infected or,in the case of bile and pancreatic juice, toxic for adjacent tissue.
Because of the potential function of abdominal drains to signal early complications,such as postoperative hemorrhage and leakage of enteric suture lines,prophylactic drainage has gained wide acceptance as a useful method to prevent complications after gastrointestinal (GI)surgery[6].Recently,some studies have called into question the benefit of routine drainage[3,4,7,8].
Cholecystectomy for symptomatic cholelithiasis is a common surgical practice in our community.It is now established that prophylactic drainage is not needed after cholecystectomy for chronic calculous cholecystitis[9,10].On the other hand,prophylactic drainage after acute calculous cholecystitis is still controversial, especially for cases with pericholecystic collections, excessive adhesions or empyema.Multiple reviews, trials and retrospective studies,in particular randomized clinical trials,have dealt with the issue whether to drain or not to drain such cases.However,the results of these trials are contradictory,deal with non-complicated cases and did not answer the clinical question in acute or complicated conditions[4,5,8].This retrospective study was conducted to answer the question whether to drain or not to drain after cholecystectomy for acute calculous cholecystitis.
PATIENTS AND METHODS
Patients
A retrospective review of all patients who underwent cholecystectomy for acute calculous cholecystitis, between April 2010 and April 2012,in Aseer Central Hospital,Abha,Saudi Arabia was done.Aseer Central Hospital is an internationally accredited hospital in which more than 400 cholecystectomy operations are performed every year representing 23%of the general surgery load of operations.Immediate cholecystectomy for acute calculous cholecystitis represents 12.5%of this load.All operations were done by consultants of general surgery with experience in the field of laparoscopic cholecystectomy.Minimal sample size needed for each group was calculated to be 37.The calculation was based on α error of 0.05,power of 0.80 with effect size 0.2.It was calculated by using G power program version 3.1.3 2007[11].
According to whether a prophylactic drain was inserted or not during the operation,patients were allocated into two groups:group A(n=38)for patients with operative drain insertion and group B(n=65) for patients without drain insertion.We included all patients fulfilling the inclusion criteria to avoid bias of selection.According to the policy of our hospital,closed suction drainage was the type of drain used in all patients of group A.Drains were removed after cholecystectomy if less than 50 mL serous/serousangionous fluid was collected during the preceding 24 hours.
Inclusion criteria were diagnosis of acute calculous cholecystitis confirmed by pathological report and patients with immediate cholecystectomy after their first episode of cholecystitis that was done in the same hospital admission.Exclusion criteria included patients who need therapeutic drainage for biliary or pancreatic leakage,or with nearby organ injury.Patients with doubtful diagnosis or with interval cholecystectomy were also excluded from the study.The protocol of the study was approved by the ethical committee of Faculty of Medicine,King Khalid University(REC# 2012-05-06).Patient consent was not required because of the retrospective nature of this study.
Data collection
Preoperative data included clinical presentation,temperature,complete blood count,and ultrasonographic findings.Operative data included excessive adhesions, bleeding,bile leak,drain insertion or not,and if they were complicated cases(peri-cholecystic collection, mucocele or empyema).Postoperative data included hospital stay,amount and nature of drained fluid,time of drain removal,drain site problems(infection,ascites, fistula,and need for secondary closure)and postoperative complications(wound infection,collection and drainage whether radiological or surgical).
Statistical analysis
The statistical analysis of data was done using the excel program for figures and SPSS(SPSS,Inc., Chicago,IL)version 16.The description of the data was done in the form of mean±SD for quantitative data and frequency and proportion for qualitative data.The analysis of the data was done to test statistical significant difference between groups.The primary endpoint was to determine if there was any difference in outcome in terms of postoperative complications(wound infection, collection necessitating drainage and reoperation)and hospital stay in cases of cholecystectomy for acute cal-culous cholecystitis with and without prophylactic drainage.For quantitative data,independent t-test was used to compare between two groups.For qualitative data Chi-square test was used.Risk adjusted analysis was done using the binary logistic regression for incidence of complications as a dependent variable and linear regression analysis for hospital stay as a dependent variable to determine the risk factors which affected the outcome if present.P<0.05 was considered significant.
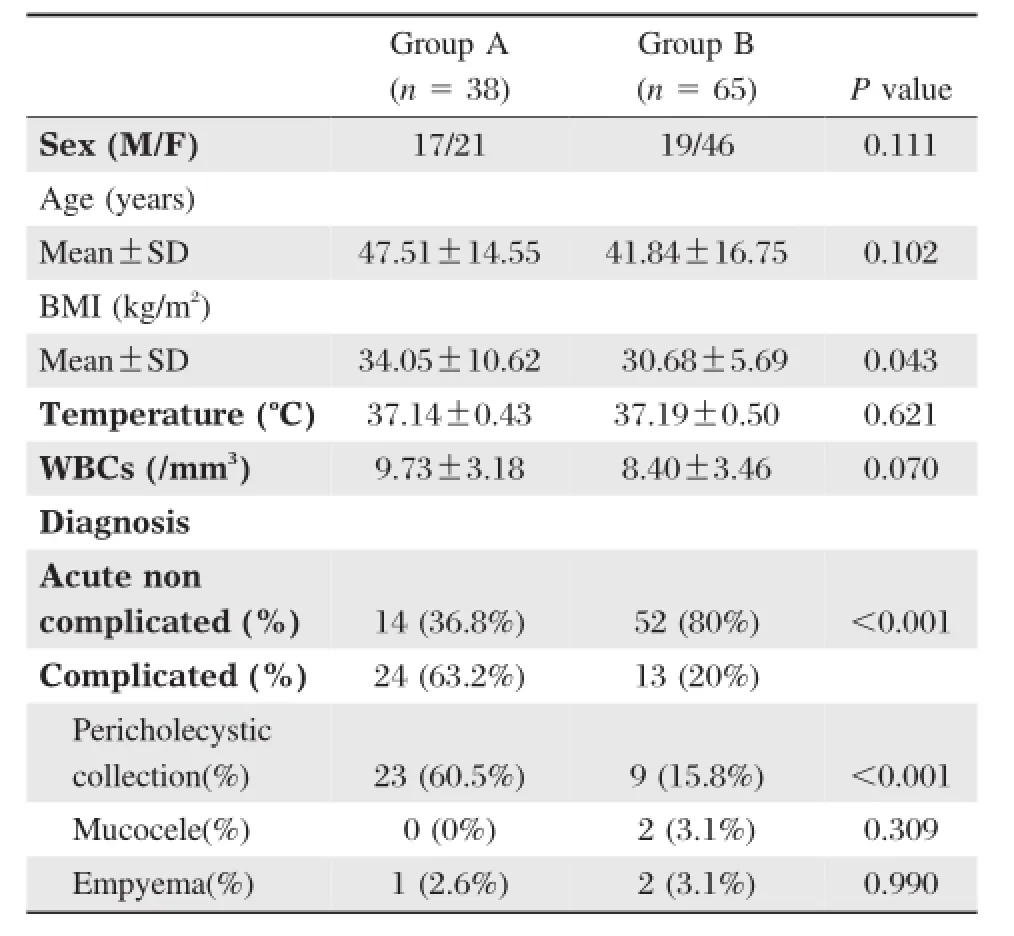
Table 1Demographic and baseline characteristics of patients undergoing cholecystectomy for acute calculous cholecystitis
RESULTS
This study included 103 patients who had cholecystectomy operation for acute calculous cholecystitis. They were allocated into two groups;group A(n= 38)for patients with operative drain insertion and group B(n=65)for patients without drain insertion. Patients in both groups were comparable regarding demographic data(Table 1).The number of patients preoperatively diagnosed as acute non-complicated cholecystitis was significantly(P≤0.001)higher in group B(80%in group B vs.36.8%in group A). Significantly more patients with pericholecystic collection were found to be in the drained group.There were more patients who were diagnosed with mucocele or empyema of the gallbladder in the undrained group, but without statistical significance.Preoperative data of the patients are shown inTable 1.
In regards to the operative data,operative time was found to be statistically longer in the drained group. All patients who were converted from laparoscopic to open cholecystectomy were in the drained group. Patients in the drained group had a mean volume of drained fluid of 49.84±34.30 mL.The nature of the drained fluid was serous or serousangious in all cases.The drain was removed after a mean time of 2.63±1.05 days.There was no significant difference between the two groups in incidence of postoperative abdominal collections necessitating drainage or wound complications.Operative and postoperative data of the patients in both groups are shown inTable 2.
Univariate analysis revealed that patients in the non-drained group had significant shorter hospital stay compared to patients in the drained group(4.48± 2.18 days in group A vs.2.50±2.20 days in group B).However,multivariate analysis(linear regression analysis of hospital stay as a dependent factor)revealed that preoperative complications,which were significantly more in the drain group(group A),were a significant factor(P<0.001)affecting hospital stay.Binary logistic regression analysis of incidence of complications as a dependent factor revealed no significant effect of different associated risk factors affecting the net results.Multivariate analyses are shown inTable 3and4.
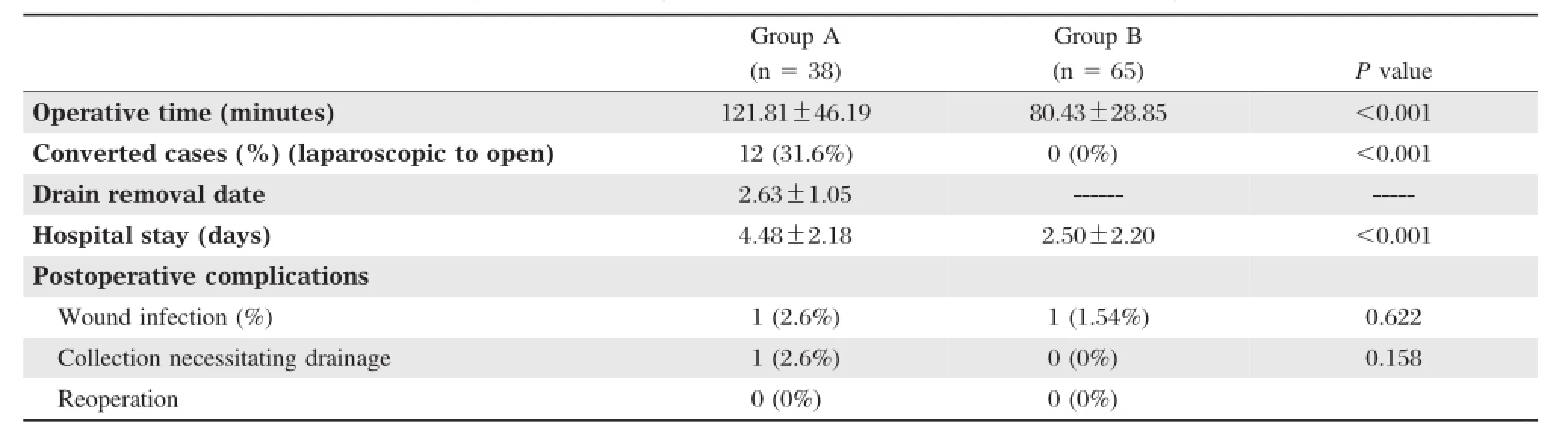
Table 2Comparison of surgical characteristics between the two groups.
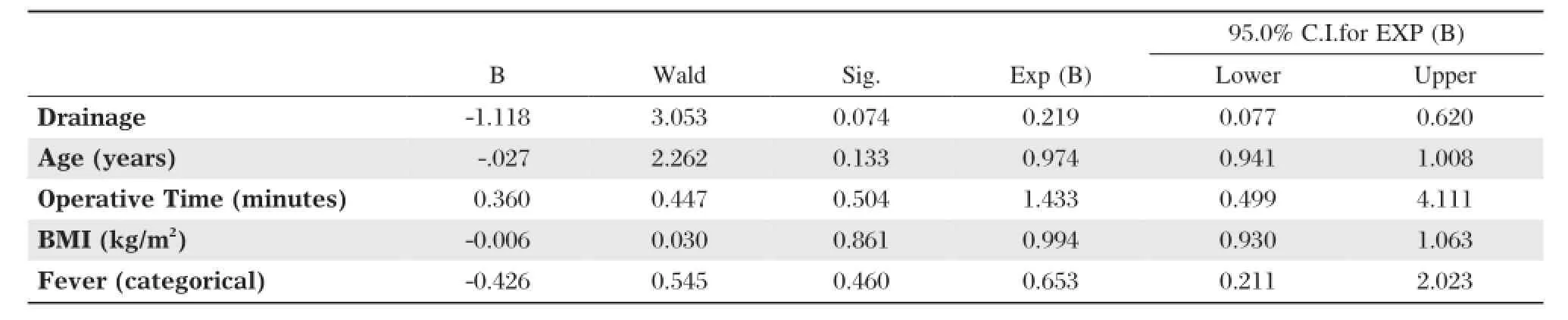
Table 3Binary logistic regression analysis of incidence of postoperative complications as a dependent variable.
DISCUSSION
Prophylactic abdominal drains have been routinely used in various abdominal surgeries without clear scientific evidence.Many surgeons still continue drainage for reasons based on traditional teaching and not on reliable facts and figures.The main motive behind this practice was the fear of missing complications such as postoperative bleeding and anastomotic leakage.Regarding cholecystectomy,the major reason for drainage is the fear of bile leakage that may lead to bile peritonitis;this is usually due to an aberrant bile duct and not slippage of the cystic duct ligature[12].Fear of blood collection requiring intervention is another reason for routine drainage after cholecystectomy[13]. Nowadays,there is consensus that there is no indication to insert a prophylactic drain after elective laparoscopic or open cholecystectomy.However,regarding cholecystectomy for acute cholecystectitis,there is still debate regarding drain insertion[9,10].
Being a retrospective study,it was not possible to know the surgeon′s justification for drain insertion, but statistical analysis revealed that the main factors which influenced the insertion of a drain were:(1) Complicated acute cholecystitis,particularly with pericholecystic collection;(2)Prolonged operative time; (3)Conversion from laparoscopic to open cholecystectomy.The results of our study showed no benefit of inserting a drain in group A,whether for non-complicated or complicated cases,compared to group B (with no drainage insertion).The presence of pericholecystic collection was treated safely in group B with thorough washing and aspiration of the washing fluid without drain insertion.We could not find evidence in the literature to support drain insertion for cases with prolonged operative time or after conversion to open cholecystectomy.
The mean drainage volume in our study was 49.84 ±34.30 mL of serousanguinous fluid.Post-cholecystectomy collections in the subhepatic recess are on the whole small,rapidly reabsorbed,and essentially similar in volume whether a drain is used or not[14].Thiebe and Eggert[15]reported that the total number of abdominal collections was higher in drained patients(44%) compared with non-drained patients(4.1%).They also suggested that the drain provokes leakage from superficial biliary ductules damaged by dissection and argued that without drainage it would rapidly wall off.In addition,drains sometimes provide a false sense of security as the drain does not guarantee either prevention or treatment of postoperative collections.The only case in this study that required postoperativeultrasound guided aspiration of subhepatic collection was from group with drain insertion.
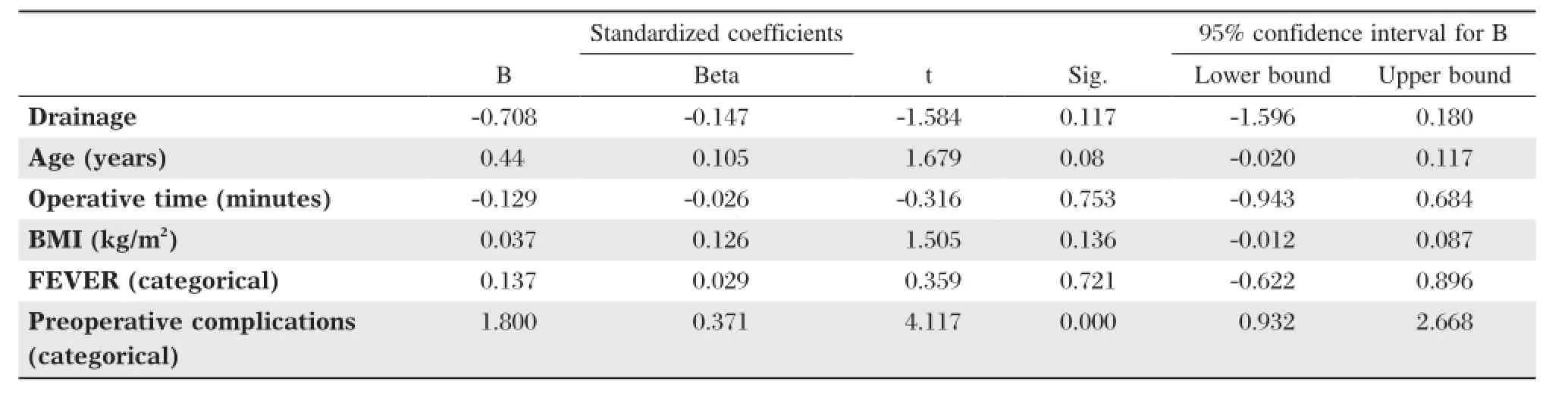
Table 4Linear regression analysis of hospital stay(days)as a dependent variable.
One justification for inserting a drainage tube after laparoscopic cholecystectomy is to deflate carbon dioxide to reduce postoperative pain,although the use of a drainage tube in these cases was found to intensify postoperative pain rather than relieving it[16,17].Many authors reported that surgically placed drains have some risk;they have been associated with increased rates of intra-abdominal and wound infection,increased abdominal pain,decreased pulmonary function,and prolonged hospital stay[16,18,19].In this study,there was no significant difference between the two groups regarding wound complications.Postoperative pain was not studied as it was not reported in the files of the patients.In regards to hospital stay,surgeons who inserted prophylactic drains waited at least 24 hours before its removal.In addition,fluid drained from the abdominal cavity was serousanguinous and was normally reabsorbed without problem.Prolongation of hospital stay usually carries the risk of nosocomial infection.In addition,it increases the cost of operation, the utilization of hospital medical resources and prolongs the waiting list of operations.
In our study,univariate analysis showed significant longer hospital stay in the drained group.But multivariate analysis was essential to clarify whether the cause of longer hospital stay was because of the drain or because of the fact that many surgeons prefer to insert prophylactic drains in complicated cases. The multivariate analysis revealed that more difficult cases were included in the drainage group,which was the cause of longer hospital stay.However,this point should be further studied in a prospective clinical study. Multivariate analysis with the incidence of postoperative complications as a dependant variable revealed no difference between the drained and non-drained group. This result clarifies the fact that prophylactic drainage added no benefit to the drained group.
Being a non-randomized,retrospective and a single center study are the main limitations of our study. These limitations may potentially bias our results. Logically,this potential bias would have been in favor of drain insertion,as drains are usually inserted in cases when complications are expected,but our study included patients with complicated and/or difficult cholecystectomies where no drains were inserted and no postoperative complications were reported.In contrast, the only case that needed postoperative drainage of collection was already in the group who had intraoperative drain insertion.
In conclusion,there was no added benefit for prophylactic drain insertion after cholecystectomy for acute calculous cholecystitis in non-complicated or in complicated cases.Further prospective randomized controlled trials are required to support our results.
ACKNOWLEDGEMENT
The authors want to thank Dr.Ahmed Abu Al Yazeed(Assistant professor of community medicine, King Khalid University)and Dr.Vinod P Singh (Associate professor of general surgery,King Khalid University)for their sincere help.
[1] Petrowsky H,Demartines N,Rousson V,Clavien PA. Evidence-based value of prophylactic drainage in gastrointestinal surgery:a systematic review and meta-analyses. Ann Surg 2004;240:1074-84.
[2] Robinson JO.Surgical drainage:a historical perspective. Br J Surg 1986;73:422-6.
[3] Moshe Schein.To Drain or not to Drain?The Role of Drainage in the Contaminated and Infected Abdomen: An International and Personal Perspective.World J Surg 2008;32:312-21.
[4] Henrik P,Nicolas D,Valentin,Pierre-Alain C.Evidencebased Value of Prophylactic Drainage in Gastrointestinal Surgery.Ann Surg 2004;240:1074-85.
[5] Mutter D,Panis Y,Escat J.Le drainage en chirurgie digestive.J Chir(Paris)1999;136:117-23.
[6] Dougherty HH,Simmons RL.The biology and practice of surgical drains.Curr Probl Surg 1992;29:559-730.
[7] Karliczek A,Jesus EC,Matos D,Castro AA,Atallah AN, Wiggers T.Drainage or nondrainage in elective colorectal anastomosis:a systematic review and meta-analysis. Colorectal Dis 2006;8:259-65.
[8] Launay-Savary M,Slim K.Analyse factuelle du drainage abdominal prophylactique.Evidence-based analysis of prophylactic abdominal drainage.Annales de chirurgie 2006;131:302-5.
[9] Gurusamy KS,Samraj K.Routine abdominal drainage for uncomplicated open cholecystectomy.Cochrane Database Syst Rev 2007,2,Art.No.:CD006003.DOI:10.1002/ 14651858.CD006003.pub2.
[10]Gurusamy KS,Samraj K,Mullerat P,Davidson BR. Routine abdominal drainage for uncomplicated laparoscopic cholecystectomy.Cochrane Database Syst Rev 2007,4,Art.No.:CD006004.DOI:10.1002/14651858. CD006004.pub3.
[11]Faul F,Erdfelder E,Lang AG,Buchner AG.Power 3:A flexible statistical power analysis program for the social, behavioral,and biomedical sciences.Behav Res Methods 2007;39:175-91.
[12]Diez JA,Pujato MR,Ferreres AR.The need of drainage after cholecystectomy.HPB Surg 1990;3:5-10.
[13]Hawasli A,Brown E.The effect of drains in laparoscopic cholecystectomy.J Laparoendosc Surg 1994;4:393-8.
[14]Shamim M.Routine Sub-hepatic Drainage versus No Drainage after Laparoscopic Cholecystectomy:Open, Randomized,Clinical Trial.Indian J Surg 2012;DOI 10.1007/s12262-012-0452-5.
[15]Thiebe U,Eggert A.Drainage after laparoscopic cholecystectomy.Minim Invasive Chir 1994;3:90-2.
[16]Uchiyama K,Tani M,Kawai M,Terasawa H,Hama T, Yamaue H.Clinical significance of drainage tube insertion in laparoscopic cholecystectomy:a prospective randomized controlled trial.J Hepatobiliary Pancreat Surg 2007;14:551-6.
[17]Picchio M,De Angelis F,Zazza S,Di Filippo A,Mancini R,Pattaro G,et al.Drain after elective laparoscopic cholecystectomy.A randomized multicentre controlled trial. Surg Endosc 2012;26:2817-22.
[18]Ammori BJ,Davides D,Vezakis A,Martin IG,Larvin M, Smith S,et al.Day-case laparoscopic cholecystectomy:a prospective evaluation of a 6-year experience.J Hepatobiliary Pancreat Surg 2003;10:303-8.
[19]Yeh CY,Changchien CR,Wang JY,Chen JS,Chen HH, Chiang JM,et al.Pelvic drainage and other risk factors for leakageafter elective anterior resection in rectal cancer patients:a prospective study of 978 patients.Ann Surg 2005;241:9-13.
Received 21 June 2013,Revised 15 July 2013,Accepted 16 January 2014,Epub 10 April 2014
?Corresponding author:Dr.WalidMAbdElMaksoud,AssistantProfessor, General Surgery Department,Faculty of Medicine,King Khalid University, Abha 61421,Saudi Arabia.Tel/Fax:00966543128555/00966-17-241-8658,
E-mail:dr.waleedmaksoud@gmail.com.
The authors reported no conflict of interests.
?2014 by the Journal of Biomedical Research.All rights reserved.
10.7555/JBR.28.20130095
 THE JOURNAL OF BIOMEDICAL RESEARCH2014年3期
THE JOURNAL OF BIOMEDICAL RESEARCH2014年3期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Analytical characteristics of a qPCR-based molecular diagnostic assay-conceptual considerations for laboratory personnel
- Position and complications of pedicle screw insertion with or without image-navigation techniques in the thoracolumbar spine: a meta-analysis of comparative studies
- Correlation of obstructive sleep apnea hypopnea syndrome with metabolic syndrome in snorers
- Class A scavenger receptor activation inhibits endoplasmic reticulum stress-induced autophagy in macrophage
- Expression of human hepatic lipase negatively impacts apolipoprotein A-I production in primary hepatocytes from Lipc-null mice
- A genetic variant in pseudogene E2F3P1contributes to prognosis of hepatocellular carcinoma